He reckons his condition has nothing to do with covid.drstrangelove » 23 Apr 2022 21:31 wrote:That Brownlow medal winner from last year.
Spewing about Jed tho. One of my favorite players. Fucken typical that he'd cop it.
Moderators: Elvis, DrVolin, Jeff
He reckons his condition has nothing to do with covid.drstrangelove » 23 Apr 2022 21:31 wrote:That Brownlow medal winner from last year.

https://twitter.com/dogvoyages/status/1 ... dMSbC_ijxAC. M. Boling
@dogvoyages
·
I wake up with my heart pounding so hard in my chest that it shakes my phone if I lean my arm against my chest and try to type at the same time.
This was not a mild, benign cardiac side effect. This is me wondering how much longer I will be alive. “Safe and effective” vaccine.
https://igorchudov.substack.com/p/moder ... e-will?s=rModerna Knew Vaccinated People Will Never Acquire Proper Immunity After Breakthrough Infections
Original Antigenic Sin was hidden from us until Apr 19, 2022
`Ever wondered why some vaccinated people seem to be having endless Covid? An interesting study came out.
This study looked at two sides of the Moderna Phase 3 vaccine trial: the vaccinated group and the control group. They looked at unvaccinated people having Covid, versus vaccinated people having so called “break-through Covid infections”.
The question that they asked, was: do the vaccinated acquire the same full-spectrum immunity as the unvaccinated?
The answer was no. Vaccinated people were much LESS likely to develop broad natural immunity, compared to unvaccinated people.
Broad Natural Immunity and Nucleocapsid Antibodies
I discuss the definition of broad spectrum immunity and explain nucleocapsid antibodies in my Nov 18 article “UK Week 42-45”. I am going to plagiarize myself and copy the text right here to make it easy for my readers:
What are these N antibodies and why am I talking about them? What’s so important?
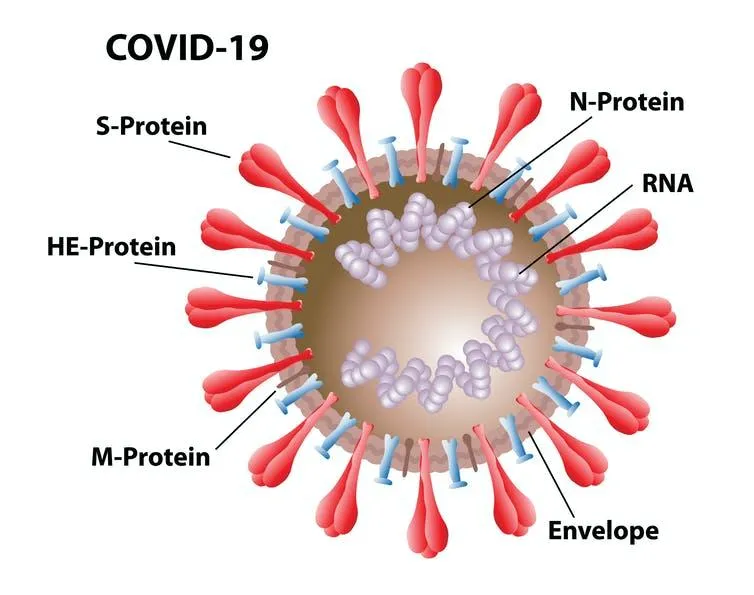
The Covid coronavirus presents numerous “epitopes” to our immune system. Those are similar to body parts in people, those are things that the virus presents to our body just as we “present” our eyes, mouths and nose.
After defeating an infection, our immune system learns to recognize these “epitopes” and reacts later, when the pathogen is reintroduced, fighting it off easier than the first time. This is the whole point of immunity.
Skipping some details, our natural, unvaccinated immunity learns to recognize the “spikes” (S-protein), the “nucleocapsid” (N-Protein) and other pieces of the virus, and develops antibodies and immune memory reacting to all of those.
This multifaceted memory also provides broader protection against “variants”.
In contrast, vaccination with any existing Covid vaccine, floods our cells with only S-protein (the “spike protein”) from a virus that only existed around January 2020. As an aside, this spike protein is extremely toxic (https://www.mdpi.com/1999-4915/13/10/2056/htm), it causes numerous side effects that we have heard about. Its effects depend on many things such as how exactly you were jabbed and how much of the vaccine entered the blood stream. S-protein can also penetrate cell nuclei and interfere with DNA repair.
Continuing, the point of “Covid vaccine” is that our immunity learns to recognize this S-protein and develops antibodies. This allows the vaccinated to fight off Covid-19 infection in the first few months post-vaccination. Then these S-antibodies decline, immunity wanes, and we end up with no immunity in the vaccinated.
What is important is that vaccine immunity ONLY creates antibodies for S-protein, but not for other proteins of the real virus, such as the N-protein. This is what the Roche N test is about: it detects presence of N-antibodies, which can only appear in survivors of actual Covid-19, which has N protein, which Covid vaccine lacks.
Thus, unvaccinated survivors of Covid19 develop a variety of antibodies, including S-antibodies (like the vaxxed), N-antibodies (never seen in vaxxed who did not have covid), etc.
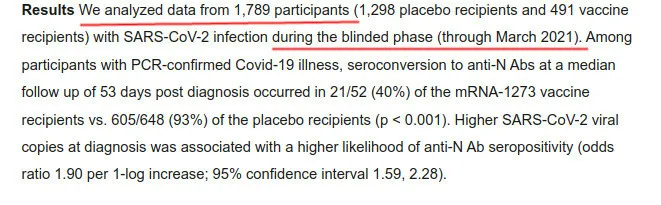
The Moderna Trial
During the original Moderna Phase 3 trial, even before Delta and Omicron, scientists found the same effect: the vaccinated are much less likely to “seroconvert” and develop the above described N antibodies. The difference between the vaccinated and the unvaccinated is FIVE TIMES, which is huge. The unvaccinated are five times more likely than the vaccinated to develop broad immunity including N antibodies.
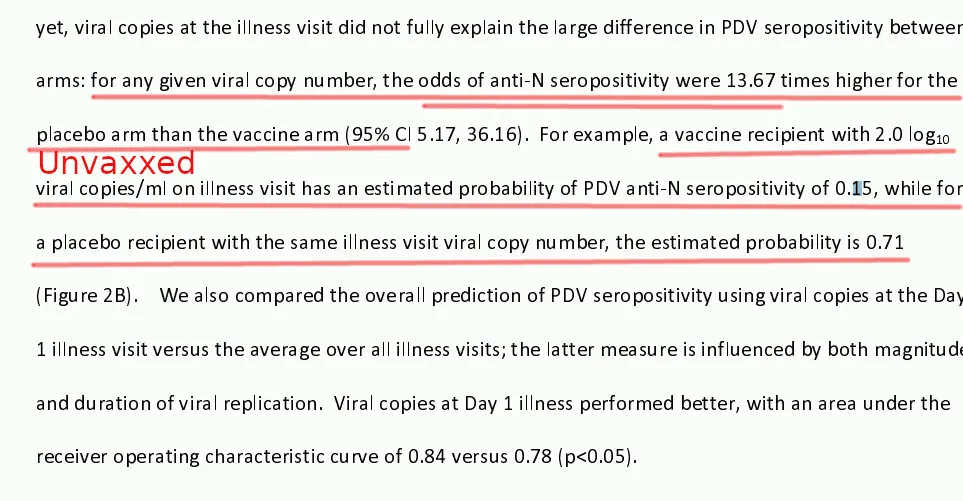
It gets even worse: for those vaccinated persons whose breakthrough infection occurred after the second dose, (illness detected on Day 29), their ability to develop N antibodies was 13 TIMES worse than that of the unvaccinated:
This inability to obtain broader natural immunity is the reason for endless covids: a covid infection in the vaccinated does not result in lasting immunity and acts similarly to an almost-worthless booster shot. A “breakthrough infection” adds a large number of temporary S-antibodies to the obsolete Wuhan virus. Whereas, the unvaccinated obtain numerous antibodies to all sorts of facets (epitopes) of the virus that infected them.
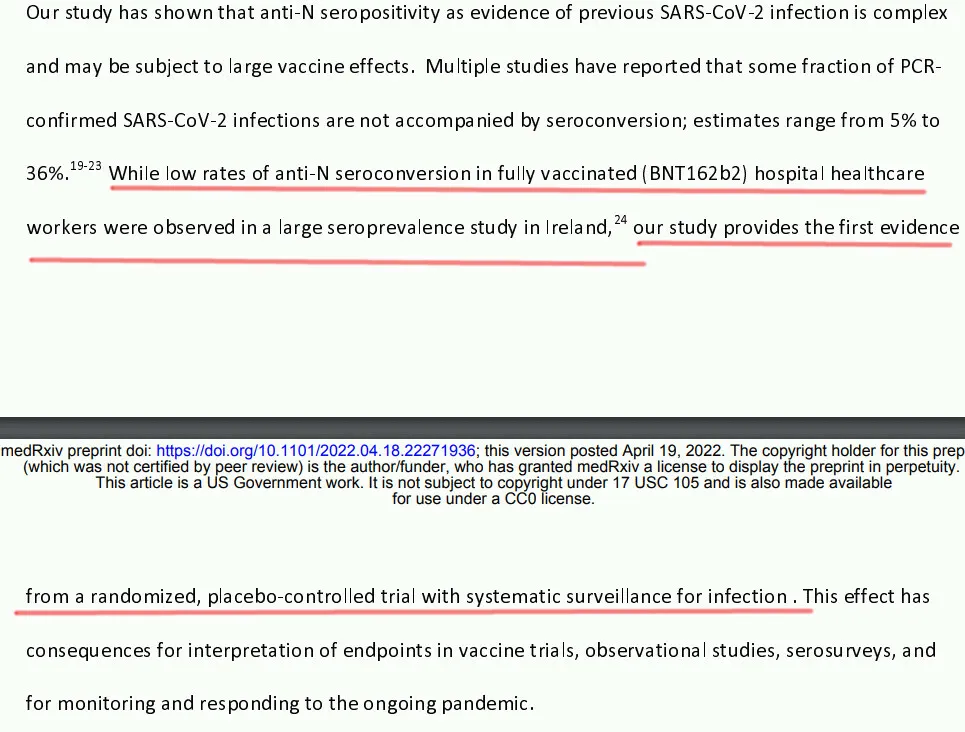
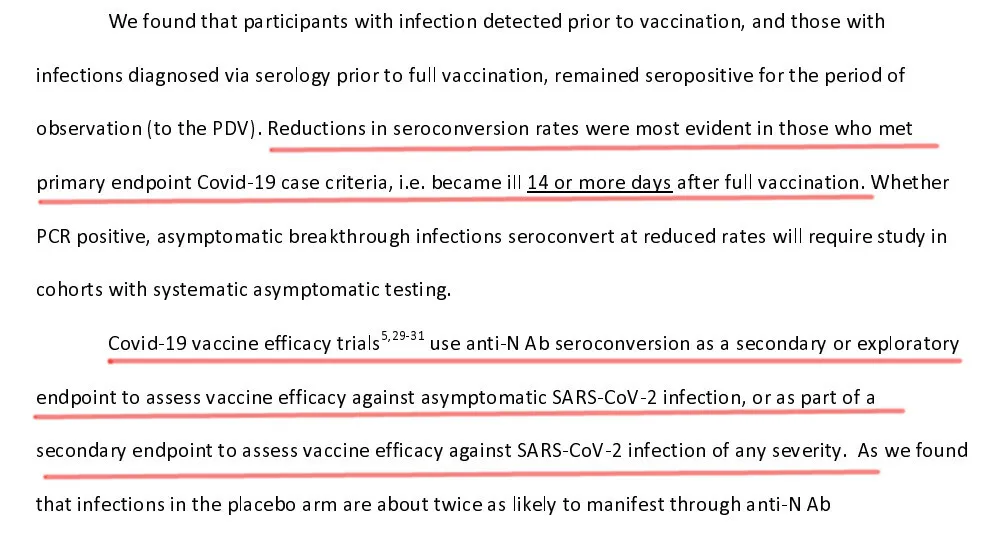
Authors also acknowledge importance of this finding and mention other studies showing the same effect:
N-Antibody Prevalence was Used for Questionable “Vaccine Effectiveness” Claims
It turns out that certain, perhaps intentionally misleading studies were using low N-antibody prevalence among the vaccinated, to falsely “prove” vaccine effectiveness. They would say “look how low is N antibody prevalence among the vaccinated!” as a proof that they do not get sick. But, as the above shows, it is not proof that they do not get sick! Sick or not, the vaccinees would NOT develop N antibodies.
What are those potentially misleading studies?
The authors mention studies 29-31. Here they are:
If you are a substack writer, take a look at them and see if you can find methodological flaws in them, based on incorrect use of N-antibody tests.
Brian Mowrey
If you like healthy disagreement, without cancel culture, note that a respected Substack writer, Brian Mowrey, does not agree with those who bring up evidence of OAS (Original Antigenic Sin). Brian is very articulate and wrote two interesting articles on the topic. I do not happen to agree with his opinion on OAS, however I respect Brian and want my readers to be exposed to his opposing point of view. Click on the above two links if you are interested. Let us know what you think.
Implications
The implications of the failure of vaccinated people to acquire full immunity are enormous. As a result of haphazardly tested vaccines, the vaccinated cannot become naturally immune after first, second, or any further infection.
Thus, any kind of herd immunity, successfully reached by low-vaccination countries, is impossible in the highly-vaccinated countries.
Endless Covid infections are NOT harmless, because Sars-Cov-2 infects immune cells and acts as a battering ram against our immune systems. Repeated blows of this “battering ram” are extremely deleterious to the immune systems of the vaccinated.
https://igorchudov.substack.com/p/sars- ... medium=web
The UK is a bit ahead of other highly vaccinated countries and has statistics exposing the depth of the problem.
https://igorchudov.substack.com/p/aids- ... medium=web
And:AIDS-Like "Chronic Covid" is Taking Over Europe, Australia and NZ
The Boosted Cannot Clear Covid Easily and Keep Getting Reinfected
https://igorchudov.substack.com/p/uk-co ... medium=web
Timing of Events
The timing of events suggests that Moderna had access to the N antibody data a very long time ago. In my opinion, a well-intentioned person who had this data, would quickly conclude that the general public deserves to be informed about OAS concerns. However, this was not done.
The data was available in or around March, 2021:
However, that study was only published now. I am NOT aware of Moderna alerting the public to this issue before. And the public had to know this, right? Please correct me if I am mistaken.
Update: Todd Zywicki mentioned that he also found some (less granular) information in Moderna’s publication of Phase 3 results, in his article dates March 10 2022. The data that he cites is very important, but it is based on a publication from Moderna that barely provided any details for N antibodies, however Todd very astutely took a note of it and reported it. I would not count that as a proper disclosure.
What do you think? Let us know in comments!
https://unglossed.substack.com/p/the-mo ... -paper?s=rThe Moderna N-Antibodies Paper
Finally, proof: Early breakthrough infections do not always generate antibodies against the Nucleocapsid protein. Well... Duh.
https://unglossed.substack.com/p/the-mo ... -probs?s=rThe Moderna Paper (Has More Prob's)
A potentially serious problem with the Moderna paper. Also: 95.4% N-positivity after Delta breakthrough infections.
https://unglossed.substack.com/p/the-mo ... mments?s=r
Igor Chudov·May 1 Liked by Brian Mowrey
>"At best, you could say that “When the Covid vaccine response is enough to keep infections mild, non-spike antibodies seem to appear less often; whereas for natural infections that are kept mild by innate immunity, non-spike antibodies appear more often.” -- But even to say this is to use early breakthrough infections as a window into what most post-Covid vaccine infections are like for only this one thing, when we know it doesn’t serve well as a window for any other aspect.
So for natural unvaxed mild infections, people make N antibodies. But for vaxed mild infections the vaxed do not make them? That IS OAS.
This is the beauty of natural immunity: have a mild illness, get long term immunity. The unvaxed do not need to have a severe illness to become immune. Thank You to wisdom of God who created us with immune systems (or Nature, for atheists). F U to the vaccine which prevents true immunity from forming.
Brian Mowrey May 1·edited
OAS is specific to the antigen. It makes no comment to unrelated antigens belonging to the same microbe. So the N antibody controversy is not even in OAS’s ballpark.
The Moderna paper demonstrates
1) The just-vaxxed “needing” less severe illness to get N antibodies. The authors just didn’t Jedi-mind-trick the data to show this, but it’s right there in 2A (HALF of seropositive placebo are above 7; HALF of seropositive vax are above 6. So the would-be high viral load half the world would get N antibodies with less viral load while the would-be low half would still have a low viral load but maybe not get N antibodies as often, IF just ignoring the other flaws that follow my “at best” statement. AND, none of this actually applies because infection efficacy is temporary and this is a distraction per 2). If all you can see is what the authors want you to see (B), you are buying into their attempt to blind you.
2) Nothing that applies to most breakthrough infections. Spring 2021 is ancient history. Footnote 6 for actual real world immune response to infection. N antibodies and non-spike T Cells are more robust for vax+infected than infected. When you teach the immune system how to say bonjour in advance, it has more capacity to learn j’ai un cheval dans ma voiture! more quickly. OAS is essentially an attempt to prove a positive (immunity smart) by assigning a negative (immunity STUPID!). It’s a fake, psy-op-y, frat bro immunity idea, and distracts from vax harm.
Igor Chudov ·May 1
This is also NOT a story about viral load explaining lack of N antibodies:
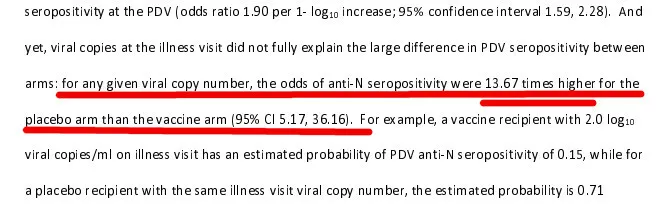
And yet, viral copies at the illness visit did not fully explain the large difference in PDV seropositivity between arms: ***for any given viral copy number, the odds of anti-N
seropositivity were 13.67 times higher for the placebo arm than the vaccine arm (95% CI 5.17, 36.16). ***
Brian Mowrey May 1
That's just statistical fabrication. Odds of N-positivity are patently, demonstrably 100% between copy numbers 5-7.5. You're letting the authors do your argument, and authors lie about their own results. This is in all science.
Igor Chudov·May 1
Okay, why would a Bill Gates funded NIAID acolyte lie to promote basically antivax ideas?
I actually see your point to some extent, but the article plainly states an antivax OAS conclusion, somewhat supported by data (maybe not to the 13.6 extent claimed but supported qualitatively).
Brian Mowrey May 1
I summed up the reasons in December, after eug banned me literally for saying "flu vaccines are also leaky." https://unglossed.substack.com/p/funeral-for-a-fact
-Reinforces the myths that older vaccines were "not leaky" or otherwise "good," depriving the overall antivax movement of new energy. Look how egm salivates over capitalism, old school vaccines, or pharma, all the time. OAS is psychic insulation for all these libertarian shibboleths. So it's intrinsically pro-pharma.
-Infects the anti-Covid-vax argument with predictions that already are or will go on to be refuted. See the rise in N antibodies in the UKHSA donor sample, refuting eug's promises in October; see footnote 6.
-Promotes boosters, as the only way to "escape" the OAS trap. See the comments section in any egm or eug OAS post. Note that this might be redundant if innate immune suppression / VAIDS are real things, and so this isn't a binary. Maybe "Hot Spot" can be taken as an argument for boosters, though I think it is more an argument for promoting innate immune health. Anyway OAS just has "aligned interests" with the (potential) truth here.
-Weakens our argument. Essentially leaves us training for a boxing match by playing with a jump rope five minutes a week. We need to be focused on vax harms, long term immune suppression, bioethics, the arenas where we will win in the end - everything but "leaky vaccine disasters."
That's not the argument posed by the above writers. They are addressing, specifically, the claims of a paper/study, and therefore their focus is on addressing the claims and/or refuting the specific claims and statements made in said study.Joe Hillshoist » Wed May 04, 2022 3:51 am wrote: The idea that covid vaccinations are bad and damage your immune system cos vaccinated people don't generate N proteins is misleading at best.
I've read that guy Igor's substack. He didn't have anything about the other external proteins not generating antibodies. Nor did he acknowledge that N-capsids against which the N Abs are formed are inside the virons and so antibodies are unable to bind to them to prevent infection.Belligerent Savant » 05 May 2022 00:41 wrote:.
There's misrepresentation intermingled in your response.
That's not the argument posed by the above writers. They are addressing, specifically, the claims of a paper/study, and therefore their focus is on addressing the claims and/or refuting the specific claims and statements made in said study.Joe Hillshoist » Wed May 04, 2022 3:51 am wrote: The idea that covid vaccinations are bad and damage your immune system cos vaccinated people don't generate N proteins is misleading at best.
Of course there are multiple types of antibodies involved in infection, and no one claimed that neutralizing antibodies are entirely protective/sterilizing. There are a number of theories as to what the absence -- or not -- of N-antibodies may mean specific to these covid mRNA products.
There are compounding issues -- multiple factors -- involved in the potential for harms as a result of mRNA/spike protein injection (including the role of synthetic LNPs and other particles), discussed at length in this thread and other threads here in RI (and elsewhere). Perhaps you can review their substack pages for more intel on their positions. Or, you can make assumptions, as you have here.
A neutralizing antibody (Ab) may block interaction of a virus protein with the host receptor10. However, a non-neutralizing Ab may even complicate the pathogenesis of some viral infections by antibody dependent enhancement (ADE). ADE is a phenomenon that is well described in viral infections, including Coronavirus11. ADE represents a paradoxical Ab effect where the virus uses the antibodies to gain access to host immune cells. Specifically, the virus uses Ab to attach to immune cells, and consequently worsen the infection through cytotoxic effects on the host immune cells12. ADE may also associated with higher viremia13. Non-neutralized viral particles may also lead to the extensive release of pro-inflammatory cytokines and the inhibition of anti-inflammatory cytokines causing immunopathology12.
The N protein of SARS-CoV2 has high homology with other highly ...pathogenic members of the coronavirus family, with a molecular weight of about 46-kDa14. Previous exposure could lead to the production of non-neutralizing Abs and establish an overwhelming pro-inflammatory state through ADE15. Patients who have higher levels of non-neutralizing IgG early in their disease may experience a worse infection due to ADE.
We hypothesize that IgG Abs against the N protein may be associated with the ADE phenomenon and higher levels of viremia. Elevated levels of coronavirus anti- N protein IgG may be associated with poorer outcomes such as increased length of hospitalization, increased likelihood of ICU admission, increased length of ICU admission, and increased mortality during hospitalization. To test these hypotheses, we conducted a prospective study on RT-PCR-confirmed COVID19 patients admitted to the University of Miami Hospital to determine clinical factors associated with poor outcomes. In addition, this study aimed to determine the association between serum SARS-CoV2 anti-N protein IgG levels and clinical outcomes of COVID19 disease. Further, we performed RT-PCR on RNA extracted from the whole blood of subjects with negative, low, and high concentrations of IgG for N-protein to detect viremia.
...
The present investigation is the first to report an association of high concentration of IgG against the N protein with poor outcome in COVID19. Prior studies reported detectable levels of total IgG in COVID19 patients in the first week of the disease23,24. We found that a high concentration of IgG against N-protein caused a threefold increase in risk of admission to the MICU. It could be theorized that N protein IgG may favor a higher inflammatory response during infection.
...
Another possible pathologic mechanism could be antibody-mediated cellular cytotoxicity in infected cells expressing N protein particles in the cell wall. Natural killer cells, neutrophils, and macrophages interact with IgG and eliminate the target cells39,40,41. Immune complex development against N protein is a fascinating potential mechanism. Berger and his colleagues showed that the immune complex induces IL6 secretion by immune cells and activates a network of proinflammatory cytokines and profound systemic inflammatory response42. Immune complex against N protein may contribute to the hyperinflammatory response that has been reported in COVID1943.

There is some evidence somewhere that N Abs contribute to ADE by enabling the virus to access T cells and other immune cells. I think, its been a while since I followed that. But the main takeaway I remember from that stuff was that N antibodies and ADE were associated with the most severe disease in non vaccinated populations.Belligerent Savant » 07 May 2022 01:12 wrote:.
You didn't address Brian Mowrey, who has a different perspective than Igor.
What's potentially causing ADE? These mRNA products, the virus, or both? One more than the other?
And again, even if that paper you cite is 100% correct, it still doesn't minimize the harms and/or inefficacy of these mRNA/adenovirus viral vector products more broadly.