How the Pandemic Will End
The U.S. may end up with the worst COVID-19 outbreak in the industrialized world. This is how it’s going to play out.
Joan Wong
Story by Ed Yong
12:53 PM ET
HEALTH
Link Copied
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here.
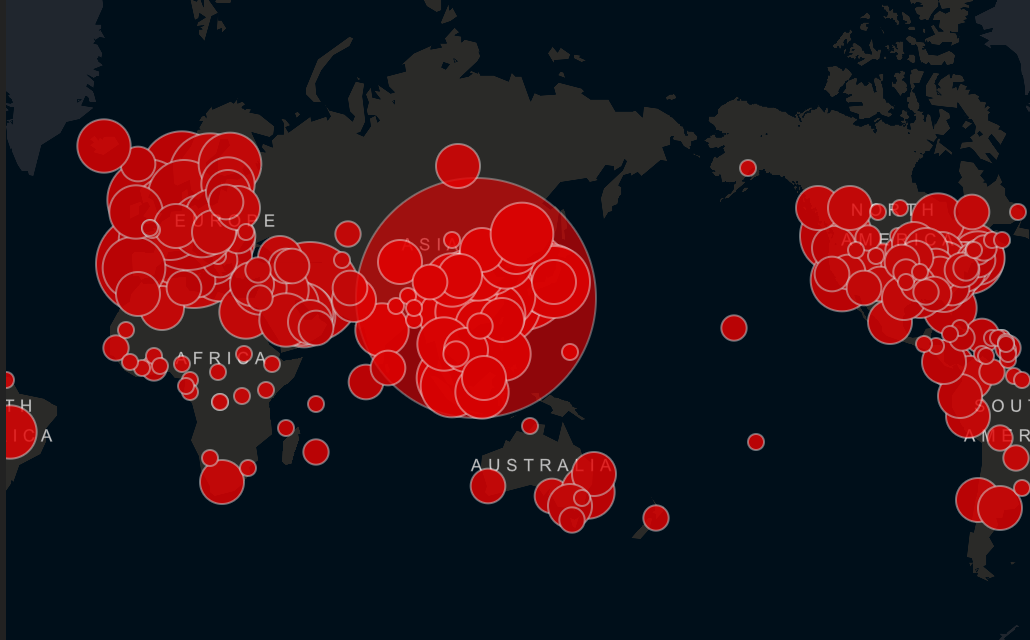
Three months ago, no one knew that SARS-CoV-2 existed. Now the virus has spread to almost every country, infecting at least 446,000 people whom we know about, and many more whom we do not. It has crashed economies and broken health-care systems, filled hospitals and emptied public spaces. It has separated people from their workplaces and their friends. It has disrupted modern society on a scale that most living people have never witnessed. Soon, most everyone in the United States will know someone who has been infected. Like World War II or the 9/11 attacks, this pandemic has already imprinted itself upon the nation’s psyche.
A global pandemic of this scale was inevitable. In recent years, hundreds of health experts have written books, white papers, and op-eds warning of the possibility. Bill Gates has been telling anyone who would listen, including the 18 million viewers of his TED Talk. In 2018, I wrote a story for The Atlantic arguing that America was not ready for the pandemic that would eventually come. In October, the Johns Hopkins Center for Health Security war-gamed what might happen if a new coronavirus swept the globe. And then one did. Hypotheticals became reality. “What if?” became “Now what?”
So, now what? In the late hours of last Wednesday, which now feels like the distant past, I was talking about the pandemic with a pregnant friend who was days away from her due date. We realized that her child might be one of the first of a new cohort who are born into a society profoundly altered by COVID-19. We decided to call them Generation C.
As we’ll see, Gen C’s lives will be shaped by the choices made in the coming weeks, and by the losses we suffer as a result. But first, a brief reckoning. On the Global Health Security Index, a report card that grades every country on its pandemic preparedness, the United States has a score of 83.5—the world’s highest. Rich, strong, developed, America is supposed to be the readiest of nations. That illusion has been shattered. Despite months of advance warning as the virus spread in other countries, when America was finally tested by COVID-19, it failed.
Anne Applebaum: The coronavirus called America’s bluff
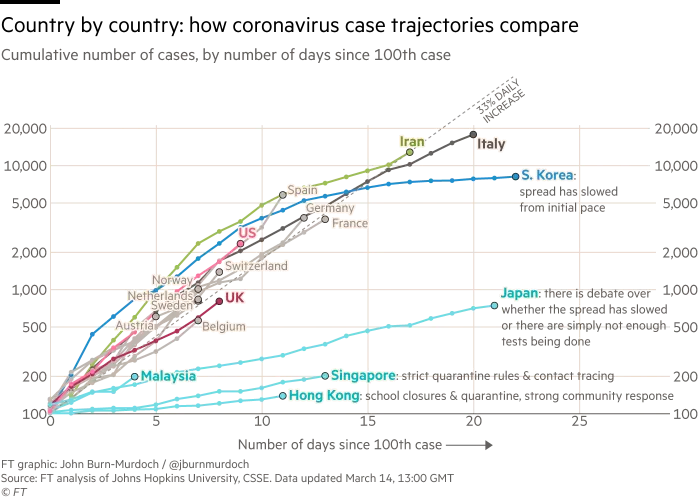
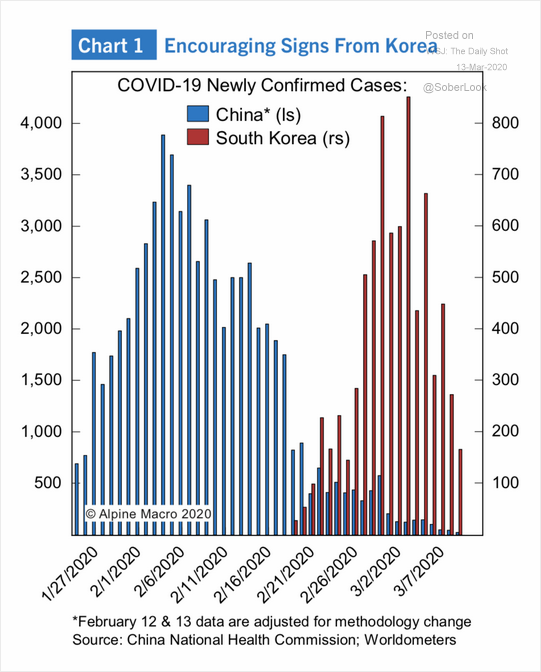
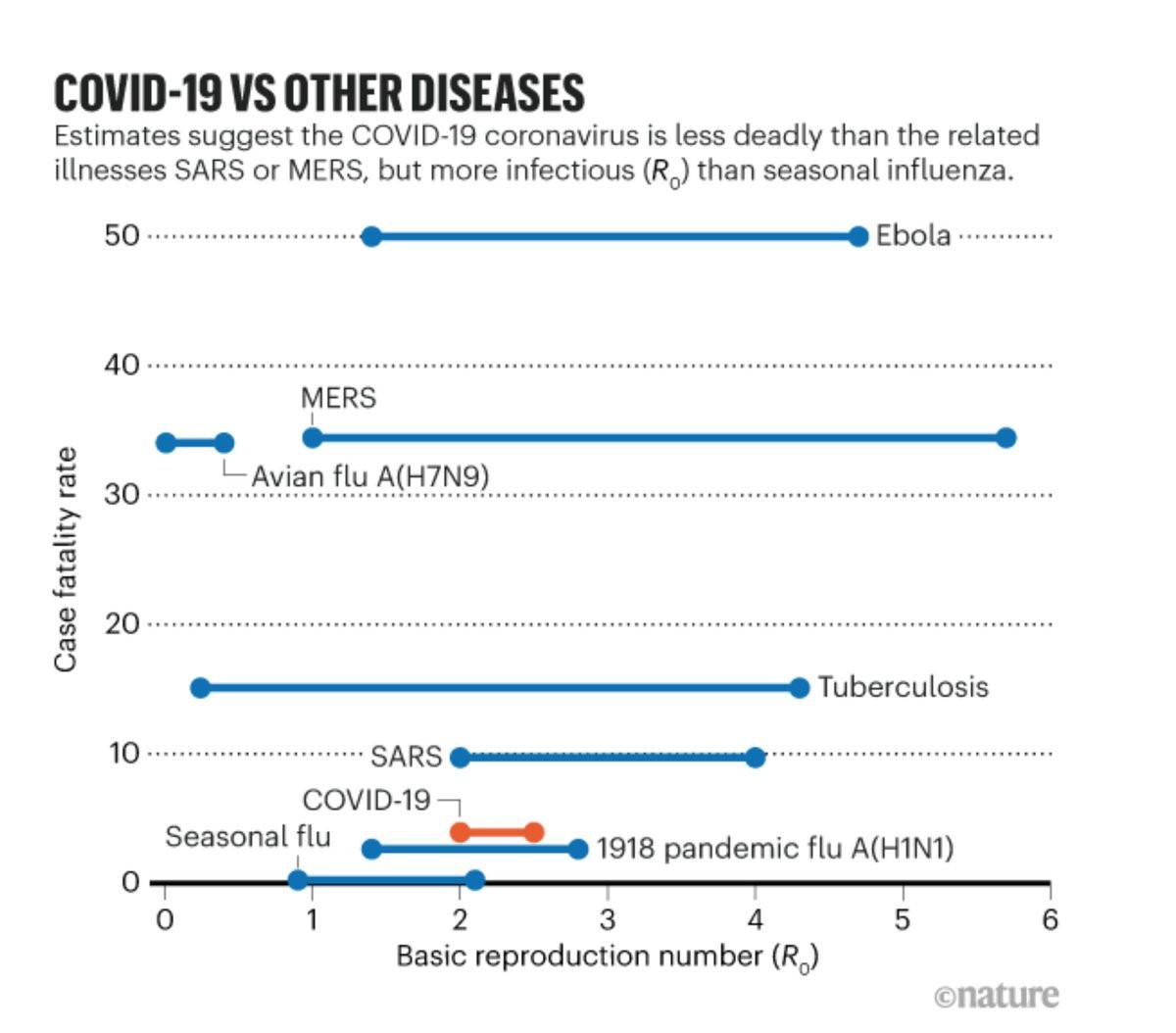
“No matter what, a virus [like SARS-CoV-2] was going to test the resilience of even the most well-equipped health systems,” says Nahid Bhadelia, an infectious-diseases physician at the Boston University School of Medicine. More transmissible and fatal than seasonal influenza, the new coronavirus is also stealthier, spreading from one host to another for several days before triggering obvious symptoms. To contain such a pathogen, nations must develop a test and use it to identify infected people, isolate them, and trace those they’ve had contact with. That is what South Korea, Singapore, and Hong Kong did to tremendous effect. It is what the United States did not.
As my colleagues Alexis Madrigal and Robinson Meyer have reported, the Centers for Disease Control and Prevention developed and distributed a faulty test in February. Independent labs created alternatives, but were mired in bureaucracy from the FDA. In a crucial month when the American caseload shot into the tens of thousands, only hundreds of people were tested. That a biomedical powerhouse like the U.S. should so thoroughly fail to create a very simple diagnostic test was, quite literally, unimaginable. “I’m not aware of any simulations that I or others have run where we [considered] a failure of testing,” says Alexandra Phelan of Georgetown University, who works on legal and policy issues related to infectious diseases.
RELATED STORIES
A hand holding an empty vial
The 4 Key Reasons the U.S. Is So Behind on Coronavirus Testing
How the Coronavirus Became an American Catastrophe
This Is How We Can Beat the Coronavirus
The testing fiasco was the original sin of America’s pandemic failure, the single flaw that undermined every other countermeasure. If the country could have accurately tracked the spread of the virus, hospitals could have executed their pandemic plans, girding themselves by allocating treatment rooms, ordering extra supplies, tagging in personnel, or assigning specific facilities to deal with COVID-19 cases. None of that happened. Instead, a health-care system that already runs close to full capacity, and that was already challenged by a severe flu season, was suddenly faced with a virus that had been left to spread, untracked, through communities around the country. Overstretched hospitals became overwhelmed. Basic protective equipment, such as masks, gowns, and gloves, began to run out. Beds will soon follow, as will the ventilators that provide oxygen to patients whose lungs are besieged by the virus.
Read: The people ignoring social distancing
With little room to surge during a crisis, America’s health-care system operates on the assumption that unaffected states can help beleaguered ones in an emergency. That ethic works for localized disasters such as hurricanes or wildfires, but not for a pandemic that is now in all 50 states. Cooperation has given way to competition; some worried hospitals have bought out large quantities of supplies, in the way that panicked consumers have bought out toilet paper.
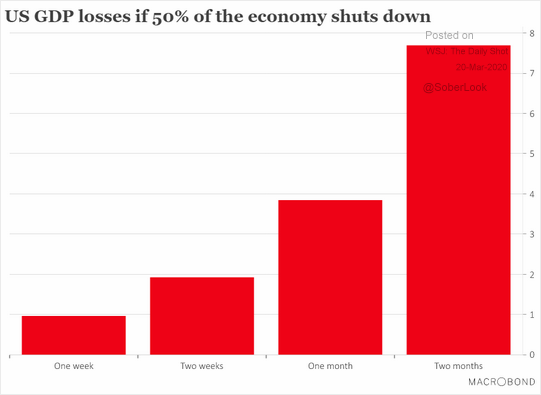
Partly, that’s because the White House is a ghost town of scientific expertise. A pandemic-preparedness office that was part of the National Security Council was dissolved in 2018. On January 28, Luciana Borio, who was part of that team, urged the government to “act now to prevent an American epidemic,” and specifically to work with the private sector to develop fast, easy diagnostic tests. But with the office shuttered, those warnings were published in The Wall Street Journal, rather than spoken into the president’s ear. Instead of springing into action, America sat idle.
Derek Thompson: America is acting like a failed state
Rudderless, blindsided, lethargic, and uncoordinated, America has mishandled the COVID-19 crisis to a substantially worse degree than what every health expert I’ve spoken with had feared. “Much worse,” said Ron Klain, who coordinated the U.S. response to the West African Ebola outbreak in 2014. “Beyond any expectations we had,” said Lauren Sauer, who works on disaster preparedness at Johns Hopkins Medicine. “As an American, I’m horrified,” said Seth Berkley, who heads Gavi, the Vaccine Alliance. “The U.S. may end up with the worst outbreak in the industrialized world.”
I. The Next Months
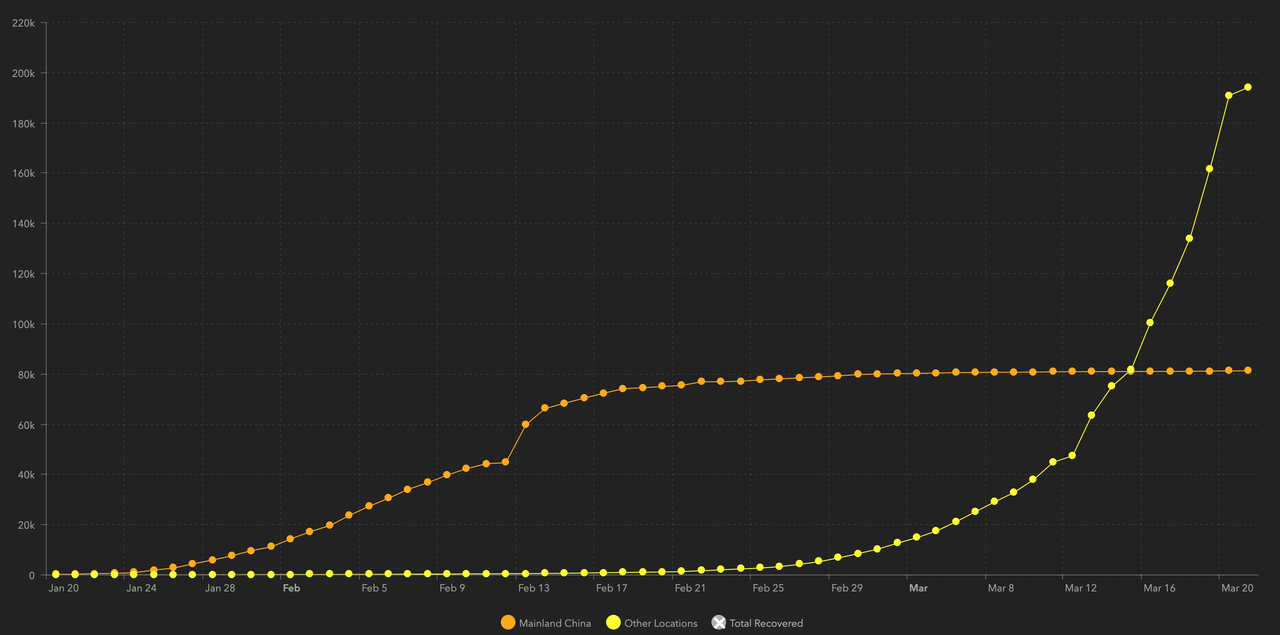
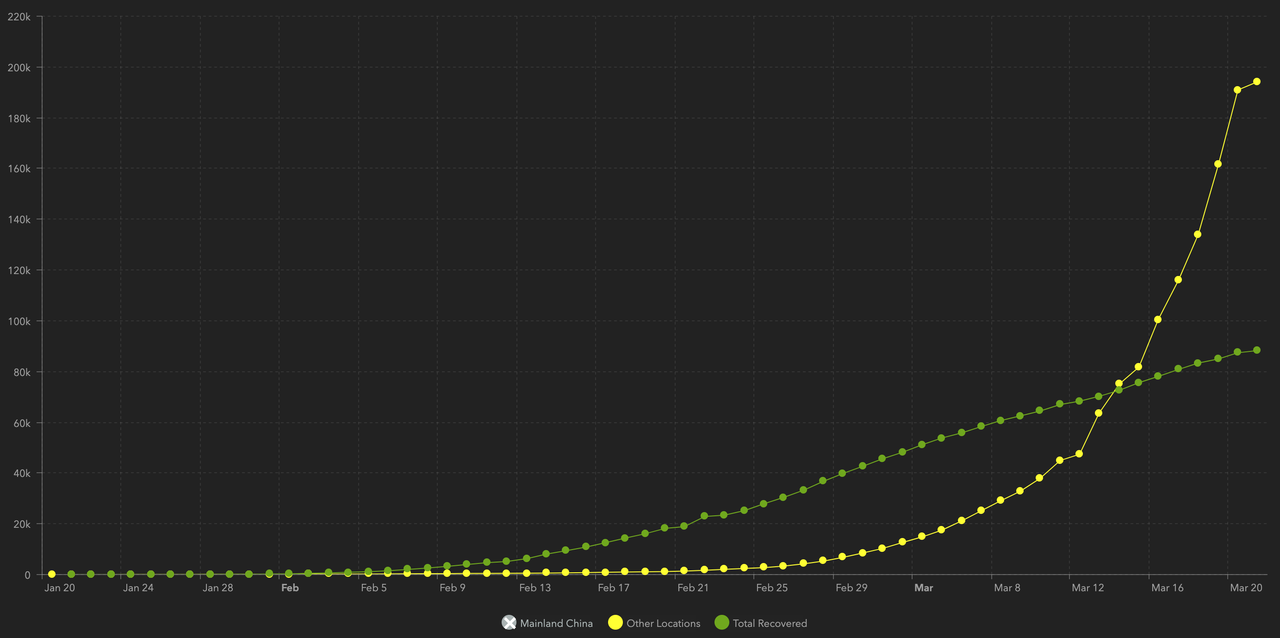
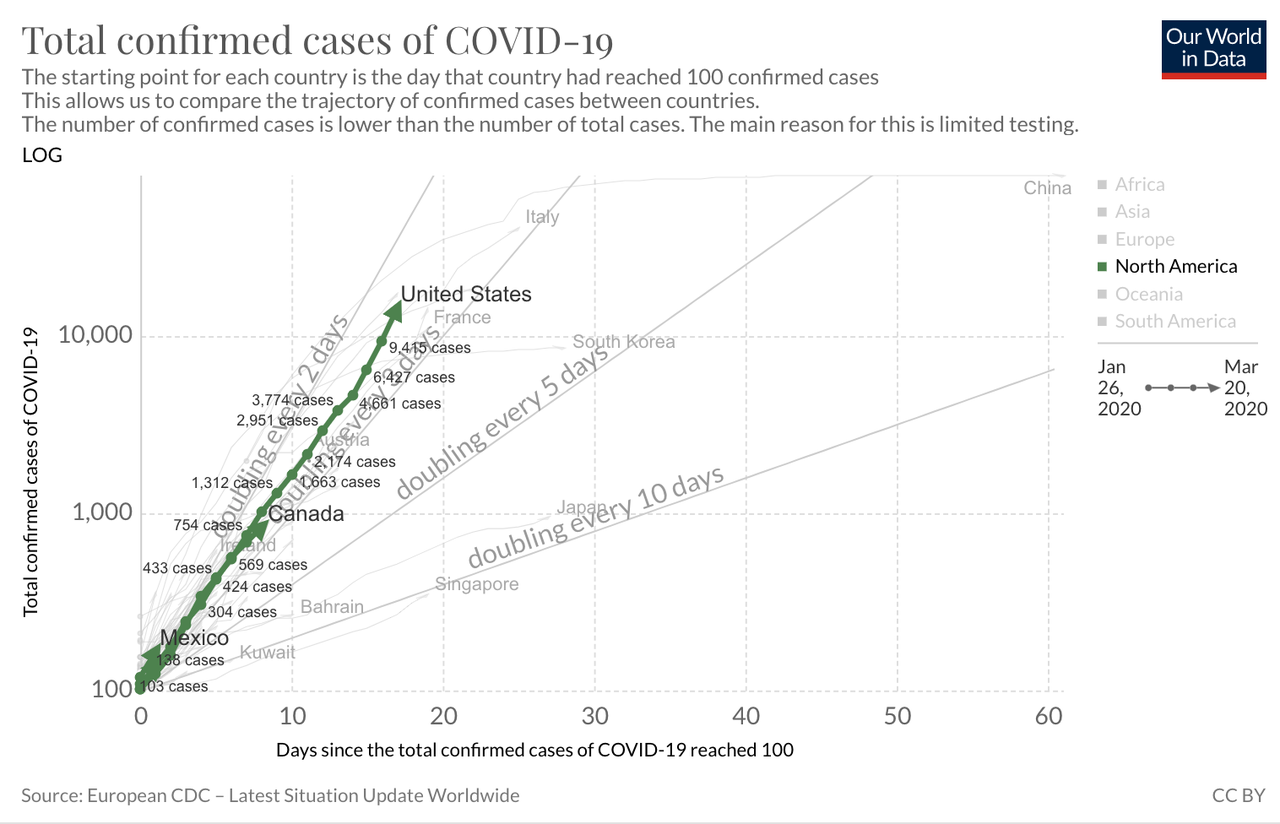
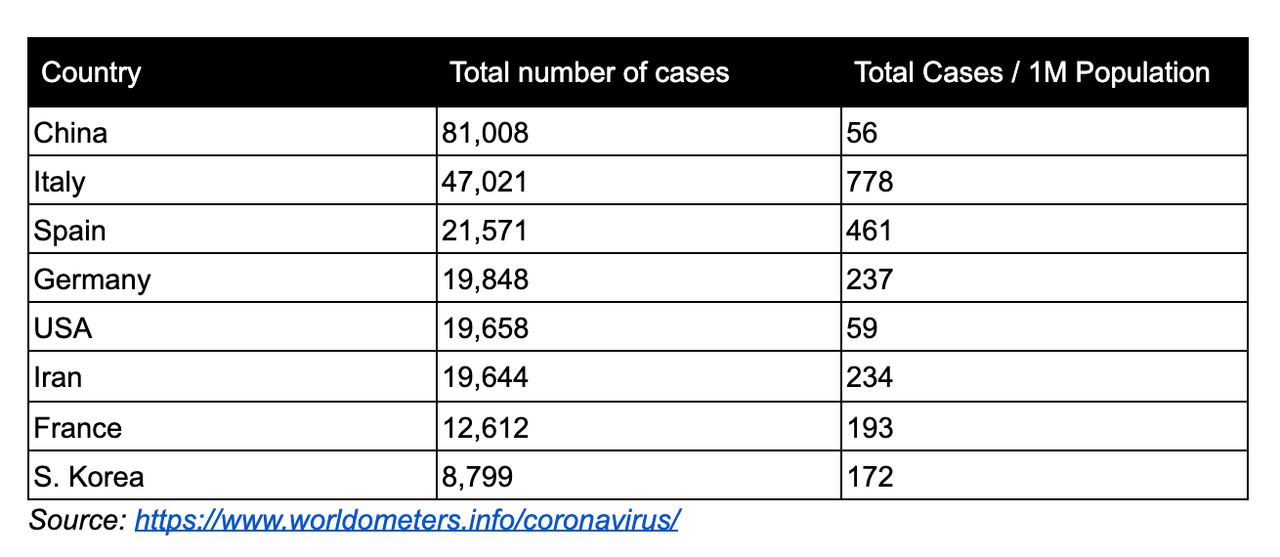
Having fallen behind, it will be difficult—but not impossible—for the United States to catch up. To an extent, the near-term future is set because COVID-19 is a slow and long illness. People who were infected several days ago will only start showing symptoms now, even if they isolated themselves in the meantime. Some of those people will enter intensive-care units in early April. As of last weekend, the nation had 17,000 confirmed cases, but the actual number was probably somewhere between 60,000 and 245,000. Numbers are now starting to rise exponentially: As of Wednesday morning, the official case count was 54,000, and the actual case count is unknown. Health-care workers are already seeing worrying signs: dwindling equipment, growing numbers of patients, and doctors and nurses who are themselves becoming infected.
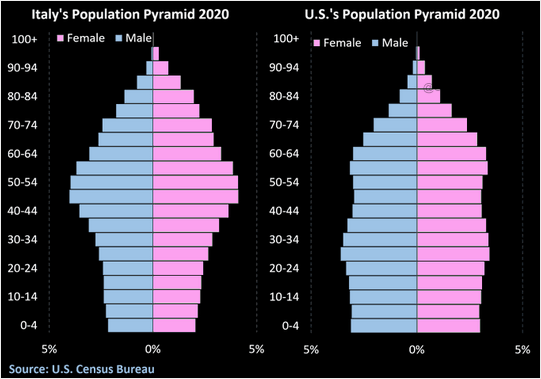
Italy and Spain offer grim warnings about the future. Hospitals are out of room, supplies, and staff. Unable to treat or save everyone, doctors have been forced into the unthinkable: rationing care to patients who are most likely to survive, while letting others die. The U.S. has fewer hospital beds per capita than Italy. A study released by a team at Imperial College London concluded that if the pandemic is left unchecked, those beds will all be full by late April. By the end of June, for every available critical-care bed, there will be roughly 15 COVID-19 patients in need of one. By the end of the summer, the pandemic will have directly killed 2.2 million Americans, notwithstanding those who will indirectly die as hospitals are unable to care for the usual slew of heart attacks, strokes, and car accidents. This is the worst-case scenario. To avert it, four things need to happen—and quickly.
Read: All the president’s lies about the coronavirus
The first and most important is to rapidly produce masks, gloves, and other personal protective equipment. If health-care workers can’t stay healthy, the rest of the response will collapse. In some places, stockpiles are already so low that doctors are reusing masks between patients, calling for donations from the public, or sewing their own homemade alternatives. These shortages are happening because medical supplies are made-to-order and depend on byzantine international supply chains that are currently straining and snapping. Hubei province in China, the epicenter of the pandemic, was also a manufacturing center of medical masks.
In the U.S., the Strategic National Stockpile—a national larder of medical equipment—is already being deployed, especially to the hardest-hit states. The stockpile is not inexhaustible, but it can buy some time. Donald Trump could use that time to invoke the Defense Production Act, launching a wartime effort in which American manufacturers switch to making medical equipment. But after invoking the act last Wednesday, Trump has failed to actually use it, reportedly due to lobbying from the U.S. Chamber of Commerce and heads of major corporations.
Some manufacturers are already rising to the challenge, but their efforts are piecemeal and unevenly distributed. “One day, we’ll wake up to a story of doctors in City X who are operating with bandanas, and a closet in City Y with masks piled into it,” says Ali Khan, the dean of public health at the University of Nebraska Medical Center. A “massive logistics and supply-chain operation [is] now needed across the country,” says Thomas Inglesby of Johns Hopkins Bloomberg School of Public Health. That can’t be managed by small and inexperienced teams scattered throughout the White House. The solution, he says, is to tag in the Defense Logistics Agency—a 26,000-person group that prepares the U.S. military for overseas operations and that has assisted in past public-health crises, including the 2014 Ebola outbreak.
This agency can also coordinate the second pressing need: a massive rollout of COVID-19 tests. Those tests have been slow to arrive because of five separate shortages: of masks to protect people administering the tests; of nasopharyngeal swabs for collecting viral samples; of extraction kits for pulling the virus’s genetic material out of the samples; of chemical reagents that are part of those kits; and of trained people who can give the tests. Many of these shortages are, again, due to strained supply chains. The U.S. relies on three manufacturers for extraction reagents, providing redundancy in case any of them fails—but all of them failed in the face of unprecedented global demand. Meanwhile, Lombardy, Italy, the hardest-hit place in Europe, houses one of the largest manufacturers of nasopharyngeal swabs.
Read: Why the coronavirus has been so successful
Some shortages are being addressed. The FDA is now moving quickly to approve tests developed by private labs. At least one can deliver results in less than an hour, potentially allowing doctors to know if the patient in front of them has COVID-19. The country “is adding capacity on a daily basis,” says Kelly Wroblewski of the Association of Public Health Laboratories.
On March 6, Trump said that “anyone who wants a test can get a test.” That was (and still is) untrue, and his own officials were quick to correct him. Regardless, anxious people still flooded into hospitals, seeking tests that did not exist. “People wanted to be tested even if they weren’t symptomatic, or if they sat next to someone with a cough,” says Saskia Popescu of George Mason University, who works to prepare hospitals for pandemics. Others just had colds, but doctors still had to use masks to examine them, burning through their already dwindling supplies. “It really stressed the health-care system,” Popescu says. Even now, as capacity expands, tests must be used carefully. The first priority, says Marc Lipsitch of Harvard, is to test health-care workers and hospitalized patients, allowing hospitals to quell any ongoing fires. Only later, once the immediate crisis is slowing, should tests be deployed in a more widespread way. “This isn’t just going to be: Let’s get the tests out there!” Inglesby says.
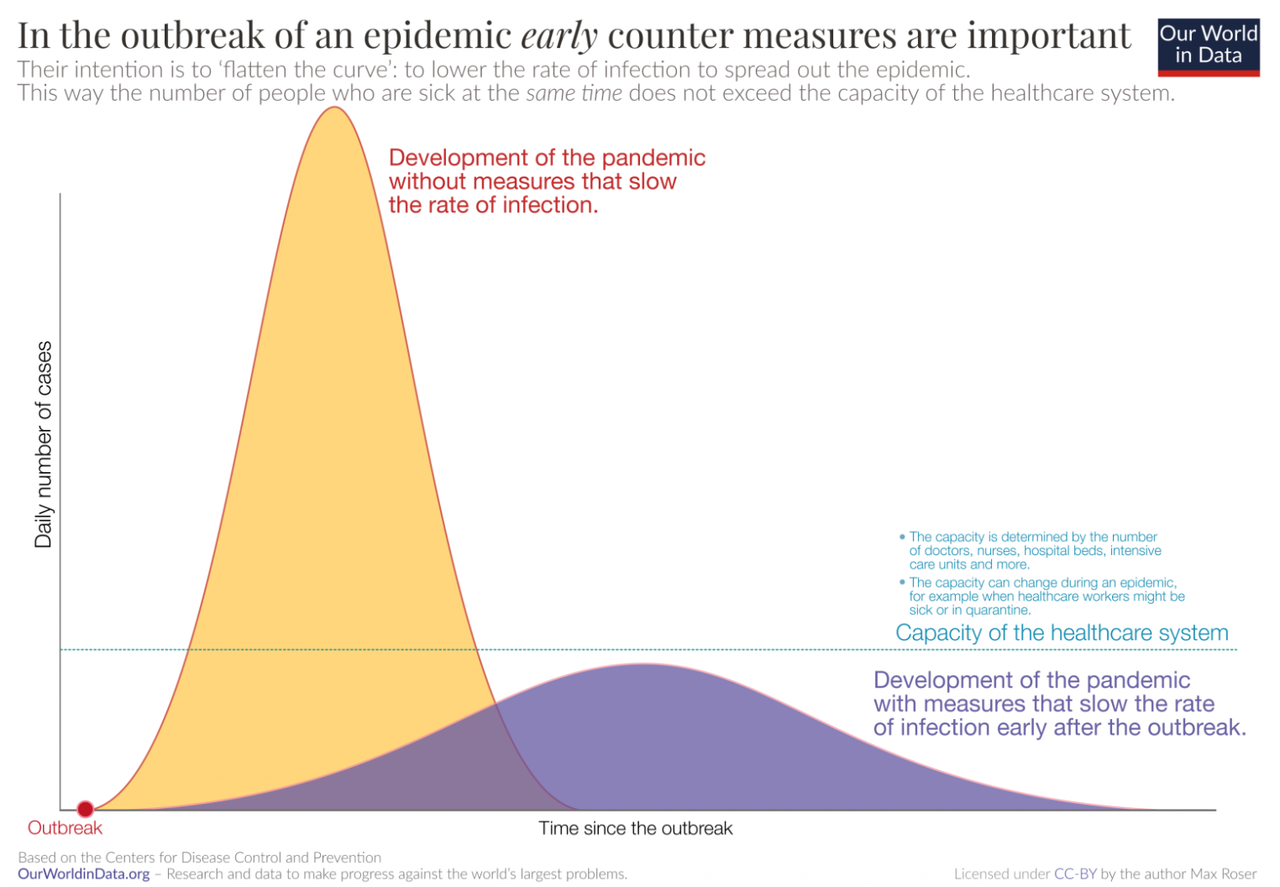
These measures will take time, during which the pandemic will either accelerate beyond the capacity of the health system or slow to containable levels. Its course—and the nation’s fate—now depends on the third need, which is social distancing. Think of it this way: There are now only two groups of Americans. Group A includes everyone involved in the medical response, whether that’s treating patients, running tests, or manufacturing supplies. Group B includes everyone else, and their job is to buy Group A more time. Group B must now “flatten the curve” by physically isolating themselves from other people to cut off chains of transmission. Given the slow fuse of COVID-19, to forestall the future collapse of the health-care system, these seemingly drastic steps must be taken immediately, before they feel proportionate, and they must continue for several weeks.
Juliette Kayyem: The crisis could last 18 months. Be prepared.
Persuading a country to voluntarily stay at home is not easy, and without clear guidelines from the White House, mayors, governors, and business owners have been forced to take their own steps. Some states have banned large gatherings or closed schools and restaurants. At least 21 have now instituted some form of mandatory quarantine, compelling people to stay at home. And yet many citizens continue to crowd into public spaces.
In these moments, when the good of all hinges on the sacrifices of many, clear coordination matters—the fourth urgent need. The importance of social distancing must be impressed upon a public who must also be reassured and informed. Instead, Trump has repeatedly played down the problem, telling America that “we have it very well under control” when we do not, and that cases were “going to be down to close to zero” when they were rising. In some cases, as with his claims about ubiquitous testing, his misleading gaffes have deepened the crisis. He has even touted unproven medications.
Away from the White House press room, Trump has apparently been listening to Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases. Fauci has advised every president since Ronald Reagan on new epidemics, and now sits on the COVID-19 task force that meets with Trump roughly every other day. “He’s got his own style, let’s leave it at that,” Fauci told me, “but any kind of recommendation that I have made thus far, the substance of it, he has listened to everything.”
Read: Grocery stores are the coronavirus tipping point
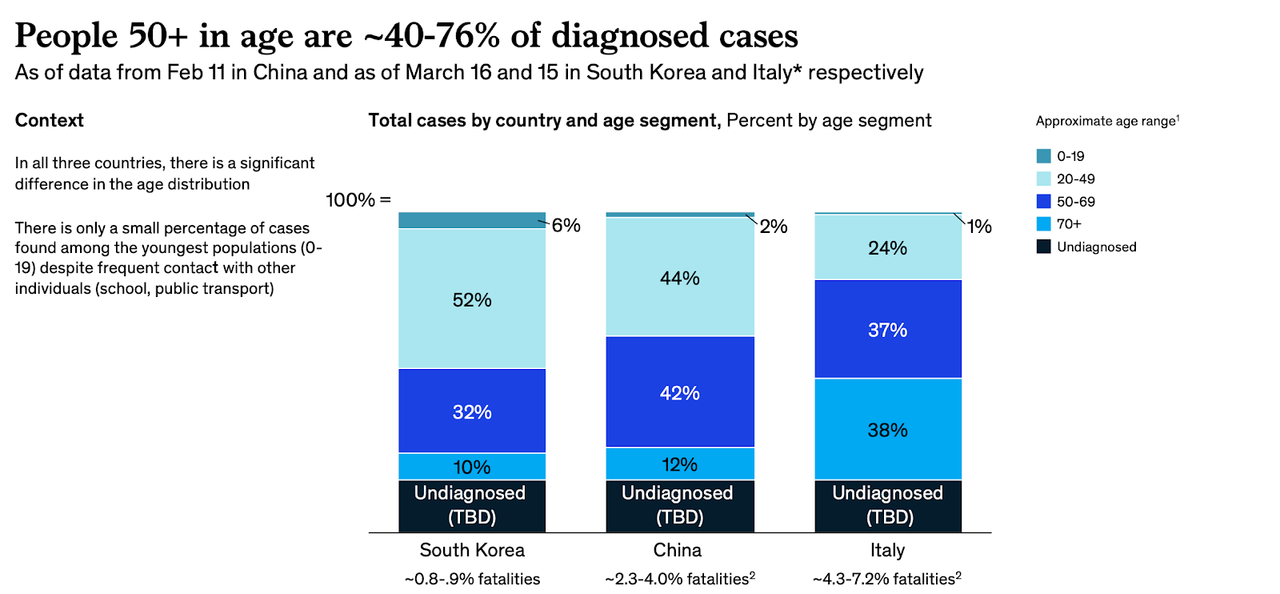
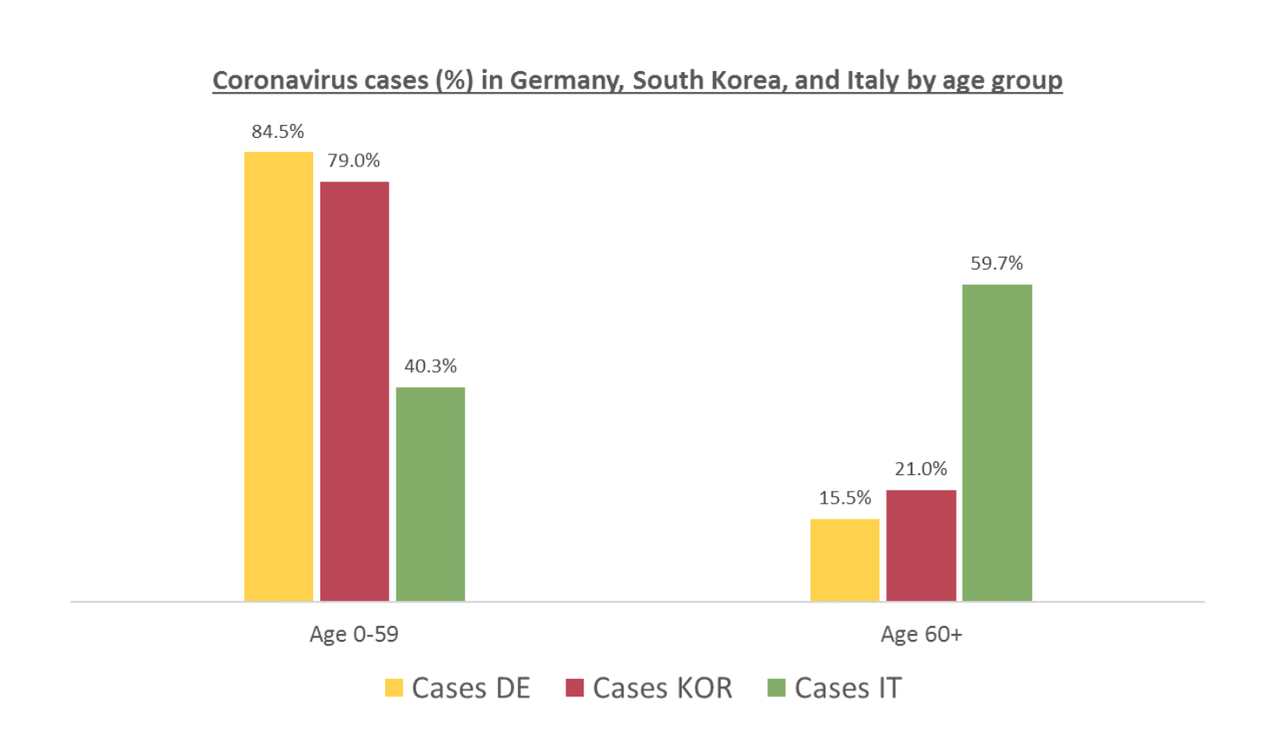
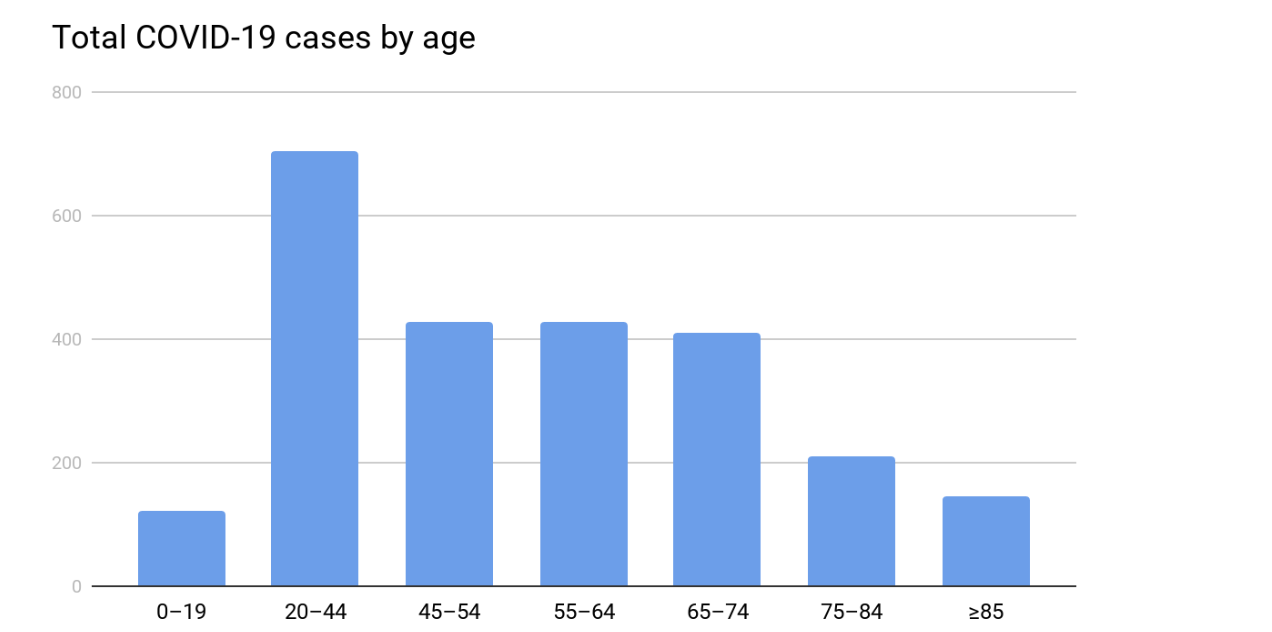
But Trump already seems to be wavering. In recent days, he has signaled that he is prepared to backtrack on social-distancing policies in a bid to protect the economy. Pundits and business leaders have used similar rhetoric, arguing that high-risk people, such as the elderly, could be protected while lower-risk people are allowed to go back to work. Such thinking is seductive, but flawed. It overestimates our ability to assess a person’s risk, and to somehow wall off the ‘high-risk’ people from the rest of society. It underestimates how badly the virus can hit ‘low-risk’ groups, and how thoroughly hospitals will be overwhelmed if even just younger demographics are falling sick.
A recent analysis from the University of Pennsylvania estimated that even if social-distancing measures can reduce infection rates by 95 percent, 960,000 Americans will still need intensive care. There are only about 180,000 ventilators in the U.S. and, more pertinently, only enough respiratory therapists and critical-care staff to safely look after 100,000 ventilated patients. Abandoning social distancing would be foolish. Abandoning it now, when tests and protective equipment are still scarce, would be catastrophic.
Read: America’s hospitals have never experienced anything like this
If Trump stays the course, if Americans adhere to social distancing, if testing can be rolled out, and if enough masks can be produced, there is a chance that the country can still avert the worst predictions about COVID-19, and at least temporarily bring the pandemic under control. No one knows how long that will take, but it won’t be quick. “It could be anywhere from four to six weeks to up to three months,” Fauci said, “but I don’t have great confidence in that range.”
II. The Endgame
Even a perfect response won’t end the pandemic. As long as the virus persists somewhere, there’s a chance that one infected traveler will reignite fresh sparks in countries that have already extinguished their fires. This is already happening in China, Singapore, and other Asian countries that briefly seemed to have the virus under control. Under these conditions, there are three possible endgames: one that’s very unlikely, one that’s very dangerous, and one that’s very long.
The first is that every nation manages to simultaneously bring the virus to heel, as with the original SARS in 2003. Given how widespread the coronavirus pandemic is, and how badly many countries are faring, the odds of worldwide synchronous control seem vanishingly small.
The second is that the virus does what past flu pandemics have done: It burns through the world and leaves behind enough immune survivors that it eventually struggles to find viable hosts. This “herd immunity” scenario would be quick, and thus tempting. But it would also come at a terrible cost: SARS-CoV-2 is more transmissible and fatal than the flu, and it would likely leave behind many millions of corpses and a trail of devastated health systems. The United Kingdom initially seemed to consider this herd-immunity strategy, before backtracking when models revealed the dire consequences. The U.S. now seems to be considering it too.
Read: What will you do if you start coughing?
The third scenario is that the world plays a protracted game of whack-a-mole with the virus, stamping out outbreaks here and there until a vaccine can be produced. This is the best option, but also the longest and most complicated.
It depends, for a start, on making a vaccine. If this were a flu pandemic, that would be easier. The world is experienced at making flu vaccines and does so every year. But there are no existing vaccines for coronaviruses—until now, these viruses seemed to cause diseases that were mild or rare—so researchers must start from scratch. The first steps have been impressively quick. Last Monday, a possible vaccine created by Moderna and the National Institutes of Health went into early clinical testing. That marks a 63-day gap between scientists sequencing the virus’s genes for the first time and doctors injecting a vaccine candidate into a person’s arm. “It’s overwhelmingly the world record,” Fauci said.
But it’s also the fastest step among many subsequent slow ones. The initial trial will simply tell researchers if the vaccine seems safe, and if it can actually mobilize the immune system. Researchers will then need to check that it actually prevents infection from SARS-CoV-2. They’ll need to do animal tests and large-scale trials to ensure that the vaccine doesn’t cause severe side effects. They’ll need to work out what dose is required, how many shots people need, if the vaccine works in elderly people, and if it requires other chemicals to boost its effectiveness.
“Even if it works, they don’t have an easy way to manufacture it at a massive scale,” said Seth Berkley of Gavi. That’s because Moderna is using a new approach to vaccination. Existing vaccines work by providing the body with inactivated or fragmented viruses, allowing the immune system to prep its defenses ahead of time. By contrast, Moderna’s vaccine comprises a sliver of SARS-CoV-2’s genetic material—its RNA. The idea is that the body can use this sliver to build its own viral fragments, which would then form the basis of the immune system’s preparations. This approach works in animals, but is unproven in humans. By contrast, French scientists are trying to modify the existing measles vaccine using fragments of the new coronavirus. “The advantage of that is that if we needed hundreds of doses tomorrow, a lot of plants in the world know how to do it,” Berkley said. No matter which strategy is faster, Berkley and others estimate that it will take 12 to 18 months to develop a proven vaccine, and then longer still to make it, ship it, and inject it into people’s arms.
Read: COVID-19 vaccines are coming, but they’re not what you think
It’s likely, then, that the new coronavirus will be a lingering part of American life for at least a year, if not much longer. If the current round of social-distancing measures works, the pandemic may ebb enough for things to return to a semblance of normalcy. Offices could fill and bars could bustle. Schools could reopen and friends could reunite. But as the status quo returns, so too will the virus. This doesn’t mean that society must be on continuous lockdown until 2022. But “we need to be prepared to do multiple periods of social distancing,” says Stephen Kissler of Harvard.
Much about the coming years, including the frequency, duration, and timing of social upheavals, depends on two properties of the virus, both of which are currently unknown. First: seasonality. Coronaviruses tend to be winter infections that wane or disappear in the summer. That may also be true for SARS-CoV-2, but seasonal variations might not sufficiently slow the virus when it has so many immunologically naive hosts to infect. “Much of the world is waiting anxiously to see what—if anything—the summer does to transmission in the Northern Hemisphere,” says Maia Majumder of Harvard Medical School and Boston Children’s Hospital.
Second: duration of immunity. When people are infected by the milder human coronaviruses that cause cold-like symptoms, they remain immune for less than a year. By contrast, the few who were infected by the original SARS virus, which was far more severe, stayed immune for much longer. Assuming that SARS-CoV-2 lies somewhere in the middle, people who recover from their encounters might be protected for a couple of years. To confirm that, scientists will need to develop accurate serological tests, which look for the antibodies that confer immunity. They’ll also need to confirm that such antibodies actually stop people from catching or spreading the virus. If so, immune citizens can return to work, care for the vulnerable, and anchor the economy during bouts of social distancing.
Scientists can use the periods between those bouts to develop antiviral drugs—although such drugs are rarely panaceas, and come with possible side effects and the risk of resistance. Hospitals can stockpile the necessary supplies. Testing kits can be widely distributed to catch the virus’s return as quickly as possible. There’s no reason that the U.S. should let SARS-CoV-2 catch it unawares again, and thus no reason that social-distancing measures need to be deployed as broadly and heavy-handedly as they now must be. As Aaron E. Carroll and Ashish Jha recently wrote, “We can keep schools and businesses open as much as possible, closing them quickly when suppression fails, then opening them back up again once the infected are identified and isolated. Instead of playing defense, we could play more offense.”
Whether through accumulating herd immunity or the long-awaited arrival of a vaccine, the virus will find spreading explosively more and more difficult. It’s unlikely to disappear entirely. The vaccine may need to be updated as the virus changes, and people may need to get revaccinated on a regular basis, as they currently do for the flu. Models suggest that the virus might simmer around the world, triggering epidemics every few years or so. “But my hope and expectation is that the severity would decline, and there would be less societal upheaval,” Kissler says. In this future, COVID-19 may become like the flu is today—a recurring scourge of winter. Perhaps it will eventually become so mundane that even though a vaccine exists, large swaths of Gen C won’t bother getting it, forgetting how dramatically their world was molded by its absence.
III. The Aftermath
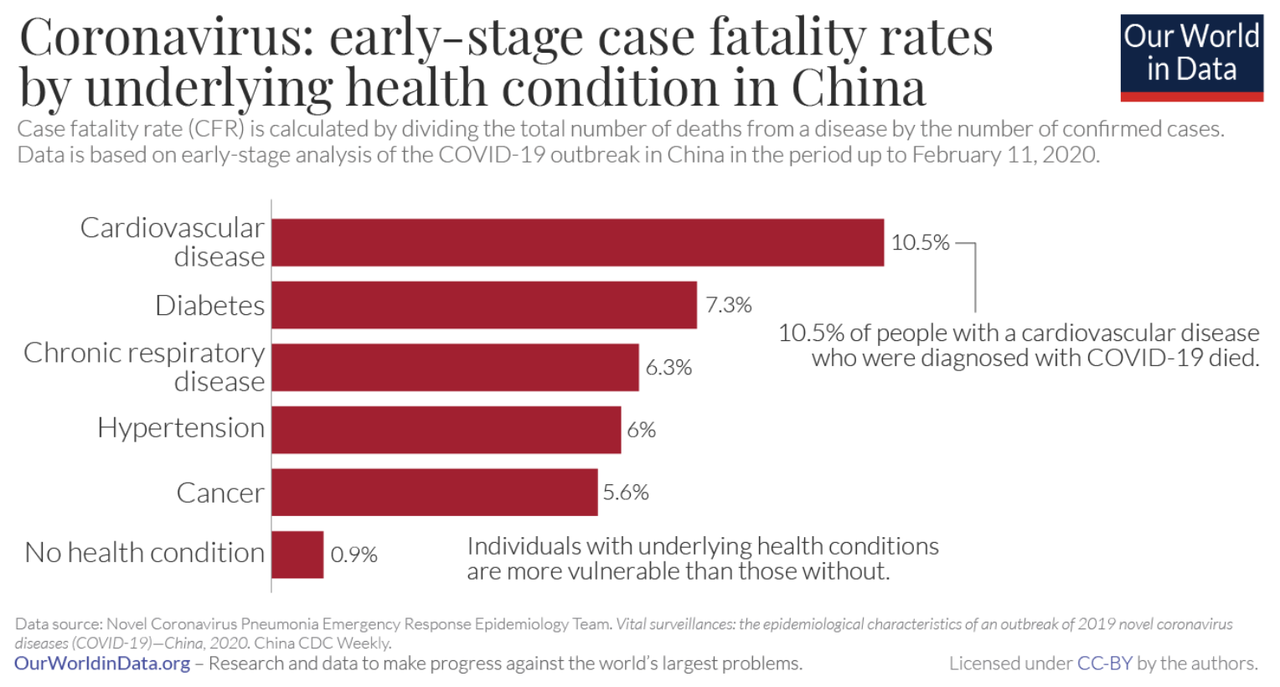
The cost of reaching that point, with as few deaths as possible, will be enormous. As my colleague Annie Lowrey wrote, the economy is experiencing a shock “more sudden and severe than anyone alive has ever experienced.” About one in five people in the United States have lost working hours or jobs. Hotels are empty. Airlines are grounding flights. Restaurants and other small businesses are closing. Inequalities will widen: People with low incomes will be hardest-hit by social-distancing measures, and most likely to have the chronic health conditions that increase their risk of severe infections. Diseases have destabilized cities and societies many times over, “but it hasn’t happened in this country in a very long time, or to quite the extent that we’re seeing now,” says Elena Conis, a historian of medicine at UC Berkeley. “We’re far more urban and metropolitan. We have more people traveling great distances and living far from family and work.”
After infections begin ebbing, a secondary pandemic of mental-health problems will follow. At a moment of profound dread and uncertainty, people are being cut off from soothing human contact. Hugs, handshakes, and other social rituals are now tinged with danger. People with anxiety or obsessive-compulsive disorder are struggling. Elderly people, who are already excluded from much of public life, are being asked to distance themselves even further, deepening their loneliness. Asian people are suffering racist insults, fueled by a president who insists on labeling the new coronavirus the “Chinese virus.” Incidents of domestic violence and child abuse are likely to spike as people are forced to stay in unsafe homes. Children, whose bodies are mostly spared by the virus, may endure mental trauma that stays with them into adulthood.
Read: The kids aren’t all right
After the pandemic, people who recover from COVID-19 might be shunned and stigmatized, as were survivors of Ebola, SARS, and HIV. Health-care workers will take time to heal: One to two years after SARS hit Toronto, people who dealt with the outbreak were still less productive and more likely to be experiencing burnout and post-traumatic stress. People who went through long bouts of quarantine will carry the scars of their experience. “My colleagues in Wuhan note that some people there now refuse to leave their homes and have developed agoraphobia,” says Steven Taylor of the University of British Columbia, who wrote The Psychology of Pandemics.
But “there is also the potential for a much better world after we get through this trauma,” says Richard Danzig of the Center for a New American Security. Already, communities are finding new ways of coming together, even as they must stay apart. Attitudes to health may also change for the better. The rise of HIV and AIDS “completely changed sexual behavior among young people who were coming into sexual maturity at the height of the epidemic,” Conis says. “The use of condoms became normalized. Testing for STDs became mainstream.” Similarly, washing your hands for 20 seconds, a habit that has historically been hard to enshrine even in hospitals, “may be one of those behaviors that we become so accustomed to in the course of this outbreak that we don’t think about them,” Conis adds.
Pandemics can also catalyze social change. People, businesses, and institutions have been remarkably quick to adopt or call for practices that they might once have dragged their heels on, including working from home, conference-calling to accommodate people with disabilities, proper sick leave, and flexible child-care arrangements. “This is the first time in my lifetime that I’ve heard someone say, ‘Oh, if you’re sick, stay home,’” says Adia Benton, an anthropologist at Northwestern University. Perhaps the nation will learn that preparedness isn’t just about masks, vaccines, and tests, but also about fair labor policies and a stable and equal health-care system. Perhaps it will appreciate that health-care workers and public-health specialists compose America’s social immune system, and that this system has been suppressed.
Aspects of America’s identity may need rethinking after COVID-19. Many of the country’s values have seemed to work against it during the pandemic. Its individualism, exceptionalism, and tendency to equate doing whatever you want with an act of resistance meant that when it came time to save lives and stay indoors, some people flocked to bars and clubs. Having internalized years of anti-terrorism messaging following 9/11, Americans resolved to not live in fear. But SARS-CoV-2 has no interest in their terror, only their cells.
Years of isolationist rhetoric had consequences too. Citizens who saw China as a distant, different place, where bats are edible and authoritarianism is acceptable, failed to consider that they would be next or that they wouldn’t be ready. (China’s response to this crisis had its own problems, but that’s for another time.) “People believed the rhetoric that containment would work,” says Wendy Parmet, who studies law and public health at Northeastern University. “We keep them out, and we’ll be okay. When you have a body politic that buys into these ideas of isolationism and ethnonationalism, you’re especially vulnerable when a pandemic hits.”
Graeme Wood: The ‘Chinese virus’ is a test. Don’t fail it.
Veterans of past epidemics have long warned that American society is trapped in a cycle of panic and neglect. After every crisis—anthrax, SARS, flu, Ebola—attention is paid and investments are made. But after short periods of peacetime, memories fade and budgets dwindle. This trend transcends red and blue administrations. When a new normal sets in, the abnormal once again becomes unimaginable. But there is reason to think that COVID-19 might be a disaster that leads to more radical and lasting change.
The other major epidemics of recent decades either barely affected the U.S. (SARS, MERS, Ebola), were milder than expected (H1N1 flu in 2009), or were mostly limited to specific groups of people (Zika, HIV). The COVID-19 pandemic, by contrast, is affecting everyone directly, changing the nature of their everyday life. That distinguishes it not only from other diseases, but also from the other systemic challenges of our time. When an administration prevaricates on climate change, the effects won’t be felt for years, and even then will be hard to parse. It’s different when a president says that everyone can get a test, and one day later, everyone cannot. Pandemics are democratizing experiences. People whose privilege and power would normally shield them from a crisis are facing quarantines, testing positive, and losing loved ones. Senators are falling sick. The consequences of defunding public-health agencies, losing expertise, and stretching hospitals are no longer manifesting as angry opinion pieces, but as faltering lungs.
After 9/11, the world focused on counterterrorism. After COVID-19, attention may shift to public health. Expect to see a spike in funding for virology and vaccinology, a surge in students applying to public-health programs, and more domestic production of medical supplies. Expect pandemics to top the agenda at the United Nations General Assembly. Anthony Fauci is now a household name. “Regular people who think easily about what a policewoman or firefighter does finally get what an epidemiologist does,” says Monica Schoch-Spana, a medical anthropologist at the Johns Hopkins Center for Health Security.
Such changes, in themselves, might protect the world from the next inevitable disease. “The countries that had lived through SARS had a public consciousness about this that allowed them to leap into action,” said Ron Klain, the former Ebola czar. “The most commonly uttered sentence in America at the moment is, ‘I’ve never seen something like this before.’ That wasn’t a sentence anyone in Hong Kong uttered.” For the U.S., and for the world, it’s abundantly, viscerally clear what a pandemic can do.
The lessons that America draws from this experience are hard to predict, especially at a time when online algorithms and partisan broadcasters only serve news that aligns with their audience’s preconceptions. Such dynamics will be pivotal in the coming months, says Ilan Goldenberg, a foreign-policy expert at the Center for a New American Security. “The transitions after World War II or 9/11 were not about a bunch of new ideas,” he says. “The ideas are out there, but the debates will be more acute over the next few months because of the fluidity of the moment and willingness of the American public to accept big, massive changes.”
One could easily conceive of a world in which most of the nation believes that America defeated COVID-19. Despite his many lapses, Trump’s approval rating has surged. Imagine that he succeeds in diverting blame for the crisis to China, casting it as the villain and America as the resilient hero. During the second term of his presidency, the U.S. turns further inward and pulls out of NATO and other international alliances, builds actual and figurative walls, and disinvests in other nations. As Gen C grows up, foreign plagues replace communists and terrorists as the new generational threat.
One could also envisage a future in which America learns a different lesson. A communal spirit, ironically born through social distancing, causes people to turn outward, to neighbors both foreign and domestic. The election of November 2020 becomes a repudiation of “America first” politics. The nation pivots, as it did after World War II, from isolationism to international cooperation. Buoyed by steady investments and an influx of the brightest minds, the health-care workforce surges. Gen C kids write school essays about growing up to be epidemiologists. Public health becomes the centerpiece of foreign policy. The U.S. leads a new global partnership focused on solving challenges like pandemics and climate change.
In 2030, SARS-CoV-3 emerges from nowhere, and is brought to heel within a month.
https://www.theatlantic.com/health/arch ... nd/608719/ED YONG is a staff writer at The Atlantic, where he covers science.