
A really good piece on the current state of affairs regarding the collection and compilation of C-19 statistics in the UK:
https://in-this-together.com/covid-19-i ... -nonsense/
(Mirrored at: https://off-guardian.org/2020/05/05/cov ... -nonsense/ )
Moderators: Elvis, DrVolin, Jeff
![]() by alloneword » Wed May 06, 2020 8:53 am
by alloneword » Wed May 06, 2020 8:53 am

![]() by alloneword » Wed May 06, 2020 9:19 am
by alloneword » Wed May 06, 2020 9:19 am
Below you will one or two updates per month on medical and political developments.
May 6, 2020
Video interviews with experts
- Stanford professor John Ioannidis explains in an interview with CNN that Covid19 is a „widespread and mild disease“ that is equally dangerous or even less dangerous than influenza (flu) for the general population. Patients in nursing homes and hospitals should receive extra protection.
- Stanford professor Dr. Scott Atlas explains in an interview with CNN that „the wrong idea of having to stop Covid19 has created a catastrophic situation in the health sector“. Professor Atlas says that the disease is „generally mild“ and that irrational fears had been created. He adds that there is „absolutely no reason“ for extensive testing in the general population, which is only necessary in hospitals and nursing homes. Professor Atlas wrote an article at the end of April entitled„The data are in – Stop the panic and end total isolation“, which generated over 15,000 comments.
- Epidemiologist Dr Knut Wittkowski explains in a new interview that the danger of Covid19 is comparable to an influenza and that the peak was already passed in most countries before the lockdown. The lockdown of entire societies was a catastrophic decision without benefits but causing enormous damage. The most important measure is the protection of nursing homes. Bill Gates‘ statements on Covid19 are „absurd“ and „have nothing to do with reality“, a vaccination against Covid19 is not necessary. The influential Covid19 model of the British epidemiologist Neil Ferguson was a „complete failure“.
- German virologist Hendrik Streeck explains the final results of his pioneering antibody study. Streeck found a Covid19 lethality of 0.36%, but explains in the interview that this is an upper limit and the lethality is probably in the range of 0.24 to 0.26% or even below. The average age of test positive deceased was approximately 81 years.
- Biology professor and Nobel Prize winner Michael Levitt, who has been analyzing the spread of Covid19 since February, describes the general lockdown as a „huge mistake“ and calls for more targeted measures, especially to protect risk groups.
- The emeritus microbiology professor Sucharit Bhakdi explains in a new German interview that politics and the media have been conducting an „intolerable fear-mongering“ and an „irresponsible disinformation campaign“ towards the population. Face masks for the general population are useless and dangerous „germ catchers“. The current crisis was brought about by the politicians themselves and has little to do with the virus. A vaccine against coronavirus is „unnecessary and dangerous“, as was the case with swine flu, and compulsory vaccination is wrong. The WHO has not taken responsibility for its many „wrong decisions“ over the years. (Note: The video was temporarily deleted by YouTube)
- The Swiss chief physician for infectiology, Dr. Pietro Vernazza, explains in a new interview that the Covid19 disease is „mild for the vast majority of people“. The „counting of infected people and the call for more tests“ would not help much. In addition, most of the people listed in the corona statistics would not die solely from Covid-19. The lethality rate of Covid-19 is „in the order of magnitude of a seasonal flu“. There is no evidence for the benefit of face masks in people who do not show symptoms themselves. (archive version)
Medical studies
- A new overview of existing PCR and antibody studies shows that the median value of Covid19 lethality (IFR) is 0.20% and thus in the range of a strong influenza.
- A new antibody study with Danish blood donors showed a very low Covid19 lethality (IFR) of 0.08% for persons under 70 years of age.
- A new antibody study from Iran, one of the earliest and most affected countries by Covid19, also showed a very low lethality of 0.08% to 0.12%.
- A new antibody study from Japan comes to the conclusion that about 400 to 800 times more people there had contact with the new coronavirus than previously thought, but showed no or hardly any symptoms. Japan had done rather few tests so far.
- A new study from Germany, with the participation of renowned virologist Christian Drosten, shows that about one third of the population already has some cellular immunity to the Covid19 corona virus, presumably through contact with earlier corona viruses (cold viruses). This cellular immunity by so-called T-cells is significantly higher than PCR and antibody tests suggested and may partly explain why many people develop no or hardly any symptoms with the new coronavirus.
- In a prison in the US state of Tennessee, only two out of 1349 test-positive people showed any symptoms at all.
- On the French aircraft carrier Charles de Gaulle, none of 1046 test-positive sailors have died so far. On the US aircraft carrier Theodore Roosevelt, one of 969 test-positive sailors has died so far (preconditions and exact cause of death are not known).
- Numerous media reported about alleged „re-infections“ of already recovered persons in South Korea. However, researchers have now come to the conclusion that all of the 290 suspected cases were false-positive test results caused by „non-infectious virus fragments“. The result again highlights the well-known unreliability of PCR virus tests.
Other medical updates
- Numerous media reported that in connection with Covid19, more and more children would fall ill with so-called Kawasaki disease (a vascular inflammation). However, the UK’s Kawasaki Disease Foundation issued a press release stating that fewer, not more, Kawasaki cases are currently being reported than usual and that of the few cases reported, only about half have tested positive for corona virus.
- In an open letter to the French Ministry of Health regarding Covid19, a French doctor speaks of „the biggest health scam of the 21st century“. The danger of the virus for the general population is in the area of influenza and the consequences of the lockdown are more dangerous than the virus itself, the French doctor argues.
- In France, it became known during a subsequent investigation that the first Covid19-positive patient had already been treated at the end of December 2019, one month earlier than previously assumed. The man was being treated for what appeared to be flu-related pneumonia. This case shows that the new corona virus either arrived in Europe earlier than assumed, or that it is not as new as assumed, or that the test result was a false-positive. In addition, it is not clear whether the man, who has long since recovered, was actually suffering from flu or corona virus or both.
- The Executive Director of the WHO recently praised Sweden as a successful model for handling Covid19. Sweden had implemented its health policy successfully and „in partnership with the population“, he said. Previously, Sweden had been heavily criticized for weeks by foreign media and politicians for its relaxed approach to Covid19.
- Belarus, which took the least action against Covid19 of all European countries and did not even cancel major events like soccer matches, is counting only 103 test-positive or suspected Covid19 deaths after more than two months. The Belarusian long-term president Lukashenko called Corona a „psychosis“.
- An extensive literature review by a Canadian researcher found that face masks do not provide protection against colds and influenza.
- A Swiss chief psychiatrist expects a sharp increase in psychological problems and more than 10,000 additional suicides worldwide due to the lockdown and unemployment.
- The so-called reproduction figure R0, which indicates the proliferation of Covid, is increasingly becoming a political issue. However, this does not change the facts: the peak of the spread was already reached in most countries before the lockdown and the reproductive rate fell to or below the stable value of one due to simple everyday and hygiene measures. The lockdown was therefore epidemiologically unnecessary.
- The clinical picture and risk groups of Covid19 corona viruses are probably related to the use of the so-called ACE2 cell receptor, which is found in the bronchi and lungs, but also in blood vessels, the intestines and kidneys. However, other coronaviruses, in particular the common cold virus NL63, also use the ACE2 cell receptor. Some researchers thus expect that the Covid19 coronavirus, too, will become a typical cold virus in the medium term.
- The exact origin of the new corona virus is still unclear. The easiest explanation remains natural transmission or mutation, which happens quite often. It is true, however, that the virological laboratory in Wuhan, as part of a research programme co-financed by the US, studied corona viruses from bats and also examined their transmissibility to other mammals, something that has been criticised for years by some researchers as too risky. The renowned head of the laboratory, however, explained that the new virus did not correspond to the corona viruses investigated in the laboratory. Earlier rumours about „bioweapons“ or „HIV sequences“ are to be regarded as disinformation in view of the relative harmlessness of the corona virus.
Nursing Homes
Nursing homes play an absolutely key role in the current corona situation. In most Western countries, 30% to 70% of all deaths „related to Covid“ occurred in nursing homes (in some regions even up to 90%). It is also known from northern Italy that the crisis there began with a panic-induced collapse of nursing care for the elderly.
Nursing homes require targeted protection and do not benefit from a general lockdown of society. If one looks only at the deaths in the general population, in most countries these are in the range of a normal or even mild wave of influenza.
Moreover, in many cases it is not clear what people in nursing homes really died of, i.e. whether it was Covid19 or stress, fear and loneliness. From Belgium, for example, it is known that about 94% of all deaths in nursing homes are untested „presumed cases“.
A new analysis of French statistics moreover shows the following: as soon as there is a „suspected case“ in a nursing home (e.g. due to coughing), all deaths are considered „suspected Covid19 deaths“, and as soon as there is a „confirmed case“ in a nursing home (even if symptomless), all deaths are considered „confirmed Covid19 deaths“.
A report from Germany vividly describes the extreme conditions under which hundreds of thousands of patients in carea and nursing homes have had to live in recent weeks, often against their will. Many of the patients were barely allowed to leave their rooms, were no longer allowed to go out into the fresh air or receive visits from their relatives.
In several nursing homes, the error-prone PCR virus test also led to serious false alarms. In one Canadian nursing home, employees fled in fear of the corona virus, resulting in the tragic death of 31 patients due to lack of care.
The former New York Times journalist and Corona critic Alex Berenson writes on Twitter: „Let’s be clear: the fact the nursing home deaths are not front and center every day in elite media coverage of COVID tells you everything you need to know about the media’s priority – which is instilling panic (and punishing Trump), not driving good health policy.
Full analysis: Mortality associated with COVID-19 outbreaks in care homes: early international evidence (LTC Covid, May 2020)Deaths in nursing homes, absolute and percentage figures (LTC Covid)
Great Britain
- Cumulative all-cause mortality in the UK is currently in the range of the five strongest flu waves in the last 25 years. The peak in daily hospital deaths was already reached on April 8 (see chart below).
- New statistical data show that in mid-April, out of about 12,000 additional deaths, about 9,000 were „related to Covid“ (including „suspected cases“), but about 3,000 were „not related to Covid“. Moreover, of the total of about 7300 deaths in nursing homes, only about 2000 were „related to Covid“. In both the „Covid19 deaths“ and the non-covid19 deaths, it is often unclear what these people actually died of. The Association of British Pathologists has therefore called for a „systematic review of the real causes of death“.
- The temporary „Nightingale“ hospitals in the UK have so far remained largely empty. A similar situation was already seen in China, the US and many other countries.
- At the end of April it became known that the lockdown was apparently not, as officially stated, recommended by a scientific commission alone, but that a high government advisor had „pushed“ the scientists to support the lockdown.
England: Test-positive deaths in hosptials (NHS)
United States
- The latest report from the US CDC shows that the Covid19 hospitalization rate among the over-65s is in the range of strong flu waves. It is slightly higher among 18 to 64-year-olds and significantly lower among those under 18.
- Video: A nurse from New York City stated in a dramatic video that New York would „murder“ Covid19 patients by putting them on invasive ventilators and destroying their lungs. The use of the invasive ventilators (instead of oxygen masks) was done „for fear of spreading the virus“. It is „a horror movie“, „not because of the disease, but because of the way it is dealt with“, the nurse explained. Experts have been warning since March against intubation of Covid19 patients.
- Dr. Daniel Murphy, the head of emergency medicine at a heavily affected hospital in New York City, recommends a quick end to the lockdown. According to Dr Murphy, the Covid19 wave had already reached its peak on April 7th. Covid19 is a serious matter, but the fear of it is exaggerated, as the vast majority of the population gets at most mildly ill. His biggest concern now is the sharp decline in the care of emergency patients and children due to the lockdown and the widespread fear in the population.
- Video: The conservative Project Veritas whistleblower platform spoke with New York funeral home directors who stated that currently Covid is written „on all death certificates“ (of suspected cases), whether there was a test or not. Many people are currently dying at home, and often the exact cause of death is no longer checked. The Covid19 statistics are inflated for political or financial reasons, the directors stated.
- The director of the Illinois Department of Health confirmed that even terminally ill people who clearly die of another cause but who test positive for Covid19 virus before or after death are recorded as Covid19 deaths.
- Due to the lockdown, 30 million people in the US have already applied for unemployment benefits by the end of April – that is significantly more than the International Labour Office ILO originally assumed for the whole world.
- Tesla boss Elon Musk called the California curfews „fascist“. The „forced imprisonment“ of people in their homes violates all their constitutional rights, Musk explained in a telephone conference.
- Video: A mother wasconfronted by police at her home because her children played illegally with neighbor children
- Video: In late April, some US media outlets were caught in a partial staging of a protest by care workers against anti-lockdown demonstrators. (Read more).
Switzerland
- Cumulative deaths since the beginning of the year in Switzerland remain within the range of a normal flu epidemic and far below the strong flu epidemic of 2015 (see graph below). Around 50% of deaths occurred in care and nursing homes.
- The Swiss government plans to transform the current corona emergency decrees into a permanent urgent federal law. Most Swiss media have not reported on this far-reaching announcement, or have done so only marginally.
- The Swiss Armed Forces began testing an app for contact tracing that is to be introduced on 11 May in collaboration with Google and Apple. Meanwhile, a Swiss „data protection office“ declared: „If the contact tracing app is suitable and necessary, it does not need to be voluntary“.
- Various vigils were held on the Swiss Bundesplatz in Berne with around 400 participants who spoke out against restrictions on constitutional rights. The rallies were cleared by the police.
- In the context of Covid19 , it was not the long-established Swiss Pandemic Commission that was used, but a newly founded „Covid-19 Task Force“, some of whose members have conflicts of interest in the pharmaceutical sector.
- Video: „Does the Swiss government belong in prison?“ Swiss journalist Reto Brennwald interviewed the entrepreneur Daniel Stricker, who temporarily fled Switzerland to Sweden in mid-March and strongly criticizes the corona policy of the Swiss government.
- A Swiss nurse has written a highly shared article on the current situation. She explains that Swiss hospitals have remained largely empty and in some cases had to furlough staff. She also says it is very unusual to transfer people over 80 years of age to intensive care units because of flu or pneumonia, where they then have to die alone instead of with their families. If this were done, the intensive care units would be overloaded almost every winter. The nurse criticises that most of the media have not sufficiently addressed the recent scientific findings on the rather low overall risk of Covid19.
Cumulative deaths compared to expected deaths, 2010 to 2020 (KW17, BFS/Stotz)
Germany and Austria
- According to a leaked protocol of the Austrian Corona Task Force, Chancellor Kurz is said to have demanded in March that the population should be „more afraid“ of infection or death of parents or grandparents. A strategy paper of the German Federal Ministry of the Interior had already become known earlier, which also called for a pychological fear campaign that was indeed implemented by politicians and the media. In retrospect, the question arises as to how many people died as a result of this largely unfounded fear.
- An open letter with already about 5000 signatures from people over 64 years of age demands: „Corona: Don’t protect us older people at this price! Let us decide for ourselves!“ For the protection of risk groups, the basic rights of the entire society should not be overridden, the authors argue.
- In Austria (and possibly also in other countries) kissing among people in love but not living together is still forbidden. This applies both in public and in one’s own flat, explained the Austrian Minister of Health.
- A German lawyer is currently suing in several courts against the government anti-corona measures, as they are „blatantly unconstitutional“.
- Videos: In Germany there have recently been several cases of serious police overreach. A young woman was brutally arrested by several police officers while shopping, as she had apparently „got 20cm too close“ to a policewoman. Another woman was instructed by the police at a rally not to hold the German constitution in front of her chest, as this was an „illegal political message“. The organizer of a peaceful rally in Berlin was also arrested in a rather brutal fasion. Even older women were arrested in a disproportionate manner. (Caution: disturbing footage of police violence).
Other updates
- The CEO of Youtube announced in an interview at the end of April that video contributions on coronavirus that contradict the guidelines of the WHO or national health authorities will be removed. For example, the video of the two skeptic Californian emergency doctors, which had over five million views, was deleted. Likewise, the interview with Professor Sucharit Bhakdi linked above was at least temporarily removed by Youtube.
- In the US magazine The Atlantic, two law professors wrote an article entitled: „Internet Speech Will Never Go Back to Normal. In the debate over freedom versus control of the global network, China was largely correct, and the U.S. was wrong.“
- Peter Hitchens: We’re destroying the nation’s wealth – and the health of millions „If you don’t defend your most basic freedom, the one to go lawfully where you wish when you wish, then you will lose it for ever. And that is not all you will lose. Look at the censorship of the internet, spreading like a great dark blot, the death of Parliament, the conversion of the police into a state militia.“
- Mathias Döpfner, CEO of Axel Springer and one of the most influential media managers in Germany, calls for a „decoupling from China“ and a strengthening of the transatlantic alliance with the USA in the wake of the Corona crisis.
- Washington Post: „The last time the government sought a ‚warp speed‘ vaccine, it was a fiasco“. The 1976 swine flu express vaccination led to paralysis and deaths.
- Looking back: Woodstock Occurred in the Middle of a Pandemic. On the rather relaxed handling of the global flu pandemic of 1968 (read more).
Covid-19 and the media
A lot of people are shocked by the dubious and often fear-mongering Covid19 reporting of many media outlets. Obviously, this is not „ordinary reporting“, but classical and massive propaganda, as it is typically employed in connection with wars of aggression or alleged terrorism.
SPR has depicted the media networks responsible for the dissemination of such propaganda in earlier infographics for the USA, for Germany and for Switzerland. Even the Internet lexicon Wikipedia is an integral part of this geopolitical media structure.
The political stance and relationship to power of different media outlets have been analyzed and compared as part of the SPR Media Navigator. This media navigator may also be helpful in evaluating the current Covid19 reporting by different media outlets.
Covid-19 and mass surveillance
By far the most significant and, from a civil society perspective, the most dangerous development in response to the coronavirus is the apparent political attempt to massively expand mass surveillance and control of society. In this context, NSA whistleblower Edward Snowden warned of the emergence of an „architecture of oppression“.
The flu-like coronavirus serves as a rationale or pretext for the introduction of strategic measures to expand monitoring and control of an increasingly revolting society. The most important instruments currently under discussion by several governments include:In the US, former President Bill Clinton discussed the introduction of a national network of „contact tracers“ with governors of various states in April. The governor of New York, Andrew Cuomo, then announced that together with billionaire and former New York City mayor Michael Bloomberg, he would create a „contact tracing army“ with up to 17,000 contact tracers for New York.
- The introduction of applications for „tracing“ contacts across society
- The establishment of units to enforce the tracing and isolation of citizens
- The introduction of digital biometric ID cards to control and regulate participation in social and professional activities.
- The extended control of travel and payment transactions (i.e. abolition of cash).
- The creation of a legal basis for access to and intervention in citizens‘ biological systems by governments or corporations (through so-called „compulsory vaccinations“).
Meanwhile, in the UK and many other countries, governments are calling for the introduction of biometric „immunity passports“ and presenting them as the allegedly „only way out“ of the primarily politically motivated lockdown. The British Tony Blair Institute called for the „expansion of technological surveillance“ to „combat the corona virus“.
In the US, the Silicon Valley data analysis company Palantir is to play a key role in setting up the data platform for monitoring the (already declining) spread of the corona virus. Palantir is known for its IT projects with intelligence agencies and the military and is headed by US billionaire and Trump supporter Peter Thiel.
In Israel, contact monitoring of the civilian population is carried out by the domestic intelligence service Shin Bet, using programs from the notorious NSO Group, known for its spy software used to monitor civil and human rights activists around the world.
Countries like Russia and China also want to massively expand the surveillance of the population in the course of „corona“, but will most likely do so independently of the US.
The idea that a pandemic can be used to expand surveillance and control of the population is not new: as early as 2010, the American Rockefeller Foundation described a „lock step scenario“ in a paper on future technological and social developments, in which current developments were anticipated with impressive accuracy (pages 18ff). At the time, the scenario was conceived as a kind of „worst case“.
Meanwhile, more than 500 scientists have warned in an open letter against „unprecedented surveillance of society“ through contact tracking apps.
The so-called Center for Health Security at Johns Hopkins University, which is at the heart of the Covid19 pandemic management and which contributed greatly to the global escalation through its misleading charts, is also very closely linked to the US security apparatus and has been involved in some of its earlier simulations and operations.
In general, cooperation with private actors to achieve geostrategic goals is not a new or unusual phenomenon in US foreign and security policy.
Microsoft founder Bill Gates, the most important private financier of the WHO and the vaccine industry, for example, financed a Global Health Program of the US Council on Foreign Relations as early as 2003, which is concerned with the question of how health policy influences geopolitics and, conversely, how it can be used to achieve geostrategic goals.
Bill Gates was also a partner of the paedocriminal multimillionaire Jeffrey Epstein, who for his part was a member and financier of the Council on Foreign Relations and had connections with US and Israeli (military) intelligence services.
![]() by alloneword » Wed May 06, 2020 12:05 pm
by alloneword » Wed May 06, 2020 12:05 pm
![]() by alloneword » Wed May 06, 2020 3:32 pm
by alloneword » Wed May 06, 2020 3:32 pm
by Sue Denim
Imperial finally released a derivative of Ferguson’s code. I figured I’d do a review of it and send you some of the things I noticed. I don’t know your background so apologies if some of this is pitched at the wrong level.
My background. I’ve been writing software for 30 years. I worked at Google between 2006 and 2014 where I was a senior software engineer working on Maps, Gmail and account security. I’ve spent the last five years at a US/UK firm where I designed the companies database product, amongst other jobs and projects. I’ve also been an independent consultant for a couple of years. Obviously I’m giving only my own professional opinion and not speaking for my current employer.
The code. It isn’t the code Ferguson ran to produce his famous Report 9. What’s been released on GitHub is a heavily modified derivative of it, after having been upgraded for over a month by a team from Microsoft and others. This codebase for instance is split into multiple files for legibility and written in C++, whereas the original program was “a single 15,000 line file that had been worked on for a decade” (this is considered extremely poor practice). A request for the original code has been made 8 days ago but ignored, it will probably take some kind of legal compulsion to make them release it. Clearly Imperial are too embarrassed by the state of it to ever release it of their own free will, which is unacceptable given it was paid for by the taxpayer and belongs to them.
The model. What it’s doing is best described as SimCity without the graphics. It attempts to simulate households, schools, offices, people and their movements etc. I won’t go further into the underlying assumptions as that’s well explored elsewhere.
Non-deterministic outputs. Due to bugs the code can produce very different results given identical inputs. They routinely act as if it’s unimportant.
This problem makes the code unusable for scientific purposes, as a key part of the scientific method is being able to replicate results. Without replication the findings might not be real at all, as the field of psychology has been finding out to its cost. Even if their original code was released it’s apparent that the same numbers as in Report 9 might not come out it.
Non-deterministic outputs may take some explanation, as it’s not something anyone previously floated as a possibility.
The documentation says, “The model is stochastic. Multiple runs with different seeds should be undertaken to see average behaviour.“
Stochastic is just a scientific sounding word for random. That’s not a problem if the randomness is intentional pseudo-randomness, i.e. the randomness is derived from a starting “seed” which is iterated to produce the random numbers. Such randomness is often used in Monte Carlo techniques. It’s safe because the seed can be recorded and the same (pseudo)random numbers produced from it in future. Any kid who’s played Minecraft is familiar with pseudo-randomness because Minecraft gives you the seeds it uses to generate the random worlds, so by sharing seeds you can share worlds.
Clearly the documentation wants us to think that given a starting seed, the model will always produce the same results.
Investigation reveals the truth – the code produces critically different results even for identical starting seeds and parameters.
I’ll illustrate with a few bugs. In issue 116 a UK “red team” at Edinburgh University reports that they tried to use a mode that stores data tables in a more efficient format for faster loading, and discovered to their surprise that the resulting predictions varied by around 80,000 deaths after 80 days:
That mode doesn’t change anything about the world being simulated so this was obviously a bug.
The Imperial team’s response is that it doesn’t matter: that they are “aware of some small non-determinisms” but “this has historically been considered acceptable because of the general stochastic nature of the model“. Note the phrasing here – Imperial know their code has such bugs but act as if it’s some inherent randomness of the universe, rather than a result of amateur coding. Apparently in epidemiology a difference of 80,000 deaths is “a small non-determinism”.
Imperial advised Edinburgh that the problem goes away if you run in single threaded mode like they do, which means they suggest to use only a single CPU core rather than the many cores any video game would successfully use. For a simulation of a country using only a single CPU core is obviously a dire problem – that’s as far from supercomputing as you can get. Nonetheless that’s how Imperial use the code: they know it breaks when they try to run it faster. It’s clear from reading the code that in 2014 Imperial tried to make the code use multiple CPUs to speed it up but never made it work reliably. This sort of programming is known to be difficult and usually requires senior, experienced engineers to get good results. Results that randomly change from run to run is a common consequence of thread safety bugs or more colloquially, Heisenbugs.
But Edinburgh come back and report that even in single threaded mode they still see the problem, so Imperial’s understanding of the issue is wrong. Finally Imperial admit there’s a bug by referencing a code change they’ve made that fixes it. The explanation given is “It looks like historically the second pair of seeds had been used at this point, to make the runs identical regardless of how the network was made, but that this had been changed when seed-resetting was implemented“. In other words in the process of changing the model they made it non-replicable and never noticed.
Why didn’t they notice? Because their code is so deeply riddled with similar bugs and they struggled so much to fix them, that they got into the habit of simply averaging the results of multiple runs to cover it up … and eventually this behaviour became normalised within the team.
In issue #30 someone reports the model produces different outputs depending what kind of computer it’s run on (regardless of number of CPUs). Again the explanation is that although this new problem “will just add to the issues” … “This isn’t a problem running the model in full as it is stochastic anyway“.
Although the academic on those threads isn’t Neil Ferguson he is well aware that the code is filled with bugs that create random results. In change #107 he authored he comments: “It includes fixes to InitModel to ensure deterministic runs with holidays enabled“. In change #158 he describes the change only as “A lot of small changes, some critical to determinacy“.
Imperial are trying to have their cake and eat it. Reports of random results are dismissed with responses like “that’s not a problem, just run it a lot of times and take the average”, but at the same time, they’re fixing such bugs when they find them. They know their code can’t withstand scrutiny so they hid it until professionals had a chance to fix it, but the damage from over a decade of amateur hobby programming is so extensive that even Microsoft were unable to make it run right.
No tests. In the discussion of the fix for the first bug Imperial state the code used to be deterministic in that place but they broke it without noticing when changing the code.
Regressions like that are common when working on a complex piece of software which is why industrial software engineering teams write automated regression tests. These are programs that run the program with varying inputs and then check the outputs are what’s expected. Every proposed change is run against every test and if any tests fail, the change may not be made.
The Imperial code doesn’t seem to have working regression tests. They tried, but the extent of the random behaviour in their code left them defeated. On 4th April they said: “However, we haven’t had the time to work out a scalable and maintainable way of running the regression test in a way that allows a small amount of variation, but doesn’t let the figures drift over time.“
Beyond the apparently unsalvageable nature of this specific codebase, testing model predictions faces a fundamental problem that the authors don’t know what the “correct” answer is until long after the fact, and by then the code has changed again anyway, thus changing the set of bugs in it. So it’s unclear what regression tests really mean for models like this even if they had some that worked.
Undocumented equations. Much of the code consists of formulas for which no purpose is given. John Carmack (a legendary video game programmer) surmised that some of the code might have been automatically translated from FORTRAN some years ago.
For example on line 510 of SetupModel.cpp there is a loop over all the “places” the simulation knows about. This code appears to be trying to calculate R0 for “places”. Hotels are excluded during this pass, without explanation.
This bit of code highlights an issue Caswell Bligh has discussed in your site’s comments: R0 isn’t a real characteristic of the virus. R0 is both an input to and an output of these models, and is routinely adjusted for different environments and situations. Models that consume their own outputs as inputs is problem well known to the private sector – it can lead to rapid divergence and incorrect prediction. There’s a discussion of this problem in section 2.2 of the Google paper, “Machine learning: the high interest credit card of technical debt“.
Continuing development. Despite being aware of the severe problems in their code that they “haven’t had time” to fix, the Imperial team continue to add new features, for instance, the model attempts to simulate the impact of digital contact tracing apps.
Adding new features to a codebase with this many quality problems will just compound them and make them worse. If I saw this in a company I was consulting for I’d immediately advise them to halt new feature development until thorough regression testing was in place and code quality had been improved.
Conclusions. All papers based on this code should be retracted immediately. Imperial’s modelling efforts should be reset with a new team that isn’t under Professor Ferguson, and which has a commitment to replicable results with published code from day one.
On a personal level I’d actually go further and suggest that all academic epidemiology be defunded. This sort of work is best done by the insurance sector. Insurers employ modellers and data scientists, but also employ managers whose job is to decide whether a model is accurate enough for real world usage and professional software engineers to ensure model software is properly tested, understandable and so on. Academic efforts don’t have these people and the results speak for themselves.
![]() by Elvis » Wed May 06, 2020 9:16 pm
by Elvis » Wed May 06, 2020 9:16 pm
https://www.economist.com/science-and-t ... -a-torrent
Scientific research on the coronavirus is being released in a torrent
Will that change how science is published?
EXPONENTIAL INCREASES are a hallmark of pandemics. The spread of SARS-CoV-2 around the world has followed such a curve inexorably. But so, too, has the research effort to understand and control the virus. More than 7,000 papers on the pandemic—covering everything from virology to epidemiology—have appeared in the past three months (see chart). A fifth of them have come out in the past week alone.
This is astonishingly fast. Researchers usually take years to design experiments, collect data and check results. Scientific journals, the self-appointed keepers of the gate between those researchers and the rest of the world, can easily take six months, often a year, to grind through the various steps of their procedure, including editing and the process of checking by anonymous outside experts, known as peer review.
The current public-health emergency has, however, turbocharged all this. With physicians, policymakers and prime ministers all needing the latest science in order to make immediate life-and-death decisions, speed has become paramount. Journals have responded to sharp rises in submissions by working overtime. In so doing they have squeezed their normal processes down to days or weeks.
Getting a move on
In the view of many, though, this is not enough. These people support a different way of disseminating scientific information—one that dethrones the journals by making journal publication an optional extra rather than a researcher’s primary goal. This model of scientific publishing relies on online repositories called preprint servers, on which papers can be posted swiftly and with only minimal formalities. Mathematicians and physicists already use them widely. Biologists increasingly do so too. Covid-19, however, has seen a step-change. Around half of the available scientific work on the pandemic has been released through preprint servers. The hope of preprinting’s supporters is that this will make the shift to using them irreversible.
Speed is good during a public-health emergency. The genome of SARS-CoV-2 was published by Chinese scientists on a public genome-data repository, a beast similar to a preprint server, just days after the virus was isolated. This permitted the rapid creation of tests to detect infections in people with suspicious symptoms. And the seriousness with which many parts of the world treated the new virus was aided by early reports which suggested that the fatality rates of the cases they looked at were much higher than those seen in influenza.
This increased speed shows that scientists have learned from their sluggish responses to previous outbreaks. In an analysis of research carried out during and after the Ebola outbreak of 2014-16 and the Zika outbreak of 2015-16, Marc Lipsitch, an epidemiologist at Harvard now working on covid-19, looked at just how sluggish those responses were. He found that, where preprints had been available, they appeared around 100 days before journal articles that had eventually been published on the same work. Unfortunately, less than 5% of all the journal articles published about the two outbreaks had been preprinted.
Dr Lipsitch recommended that preprints form a bigger part of a faster information “ecosystem” during future emergencies. And his wish, it appears, has been granted. The two biggest relevant preprint servers for covid-19 are bioRxiv, set up in 2013, and medRxiv, launched in 2019, both of which are run by Cold Spring Harbor Laboratory in New York state. (The “x” in the names represents the Greek letter “chi”, making them pronounceable as “bioarchive” and “medarchive”.)
BioRxiv is for general biological and related sciences. MedRxiv is focused on health and medicine. As The Economist went to press the two servers featured, between them, 2,853 articles about SARS-CoV-2 or covid-19. Another 789 had been posted on arXiv—at 29 years of age, the granddaddy of preprint servers—which belongs to Cornell University and specialises in maths and physical sciences.
Anyone can submit a manuscript to one of these servers and see it made available to the world within hours. Submissions are given a cursory check, to weed out opinion pieces and to ensure that they have the parts expected of a scientific paper—an abstract and sections describing methods and results. If the topic is controversial, the checkers may flag up outlandish claims. But beyond this they do not attempt to review the scientific contents of the paper. Once a preprint is online, anyone with access to the internet can read it and, if they so wish, leave detailed comments.
Fast and loose?
This process—essentially a free-for-all version of peer review—can be brutal. But it often works. Conspiracy theories about SARS-CoV-2 being an artificial, laboratory creation were fuelled by a preprint posted to bioRxiv in January, by Indian scientists. This claimed “uncanny” similarities between the genetic sequences of SARS-CoV-2 and HIV, the cause of AIDS. The study was torn apart as soon as it appeared, though, by other researchers who weighed in and pointed out serious methodological flaws. As a consequence, the manuscript has now been withdrawn.
This incident does, however, highlight a repeated criticism of preprint posting, which is that dodgy material may be misused, either accidentally or deliberately, by overzealous patients, politicians, journalists or just plain troublemakers. It is certainly a risk. But in the opinion of many, that risk does not outweigh the advantage of the free and fast flow of information between researchers that preprints provide.
For those who question the quality of science contained in preprints, there is reassurance in a recent study by researchers in Brazil (itself posted as a preprint), in which the authors used a questionnaire to score the quality of preprints on bioRxiv, and also the subsequent peer-reviewed-journal versions of these papers. They found that the journal papers were indeed of higher quality. But the difference was, on average, only 5%.
In any case, peer review as organised by journals is not perfect. It will neither pick up all errors nor weed out all bad research. The distracting focus on hydroxychloroquine as a potential covid-19 treatment was, for example, partly stimulated by a peer-reviewed paper in the International Journal of Antimicrobial Agents that was published on March 20th by French scientists. That paper now has question-marks over its rigour and reliability.
Moreover, even when a peer-reviewed paper is withdrawn, the damage may already have been done. On March 9th the South China Morning Post, an English-language newspaper in Hong Kong, published an article about research reported in Practical Preventive Medicine, a peer-reviewed journal, with a headline that read “coronavirus can travel twice as far as official safe distance”. This article has been shared more than 53,000 times on social media. Unfortunately, the study in question was retracted the day after the newspaper article was published. The Post reported the retraction immediately, but that report was shared less than 1,000 times.
The current pandemic highlights further limitations of the way peer review is typically organised. It works well when confined within a narrow group of specialists, but runs into problems when different fields rub up against each other. As Ivan Oransky, a founder of Retraction Watch, which catalogues bad practice in scientific research, observes, “if you were to do a study of the impact of social distancing, for example, and you only asked public health researchers to review that, there’s a reasonable chance that you would almost exclude or at least certainly not emphasise the economic disruption. Whereas if you only ask economists to look at it, you would almost certainly de-emphasise the health risks.”
Conventional journals might struggle to analyse the wide range of trade-offs from different angles in a situation like this. Preprints, says Dr Oransky, permit experts of different stripes to contribute, publicly and in parallel, to a wide-ranging criticism of a piece of research.
As Stuart Taylor, publishing director of the Royal Society, Britain’s top scientific academy, observes, moves towards more open science, preprints and faster dissemination of results were under way before the covid-19 pandemic. But these events will heighten those changes and probably make them permanent. Scholarly communication seems to be at an inflection point. Like many other things until recently taken for granted, it may never return to the way it was before SARS-CoV-2 came along.
![]() by fruhmenschen » Fri May 08, 2020 7:26 pm
by fruhmenschen » Fri May 08, 2020 7:26 pm
![]() by alloneword » Sat May 09, 2020 6:12 pm
by alloneword » Sat May 09, 2020 6:12 pm
..what is so unusual about the virus that produces the disease that provoked the lockdown?
The clue is right under our noses...
![]() by alloneword » Sun May 10, 2020 7:58 am
by alloneword » Sun May 10, 2020 7:58 am
alloneword » Wed May 06, 2020 8:32 pm wrote:Code Review of Ferguson’s Model:
Second Analysis of Ferguson’s Model
by Sue Denim (not the author’s real name)
I’d like to provide a followup to my first analysis. Firstly because new information has come to light, and secondly to address a few points of disagreement I noticed in a minority of responses.
The hidden history. Someone realised they could unexpectedly recover parts of the deleted history from GitHub, meaning we now have an audit log of changes dating back to April 1st. This is still not exactly the original code Ferguson ran, but it’s significantly closer.
Sadly it shows that Imperial have been making some false statements.
- ICL staff claimed the released and original code are “essentially the same functionally”, which is why they “do not think it would be particularly helpful to release a second codebase which is functionally the same”.
In fact the second change in the restored history is a fix for a critical error in the random number generator. Other changes fix data corruption bugs (another one), algorithmic errors, fixing the fact that someone on the team can’t spell household, and whilst this was taking place other Imperial academics continued to add new features related to contact tracing apps.
The released code at the end of this process was not merely reorganised but contained fixes for severe bugs that would corrupt the internal state of the calculations. That is very different from “essentially the same functionally”.- The stated justification for deleting the history was to make “the repository rather easier to download” because “the history squash (erase) merged a number of changes we were making with large data files”. “We do not think there is much benefit in trawling through our internal commit histories”.
The entire repository is less than 100 megabytes. Given they recommend a computer with 20 gigabytes of memory to run the simulation for the UK, the cost of downloading the data files is immaterial. Fetching the additional history only took a few seconds on my home WiFi.
Even if the files had been large, the tools make it easy to not download history if you don’t want it, to solve this exact problem.
I don’t quite know what to make of this. Originally I thought these claims were a result of the academics not understanding the tools they’re working with, but the Microsoft employees helping them are actually employees of a recently acquired company: GitHub. GitHub is the service they’re using to distribute the source code and files. To defend this I’d have to argue that GitHub employees don’t understand how to use GitHub, which is implausible.
I don’t think anyone involved here has any ill intent, but it seems via a chain of innocent yet compounding errors – likely trying to avoid exactly the kind of peer review they’re now getting – they have ended up making false claims in public about their work.
Effect of the bug fixes. I was curious what effect the hidden bug fixes had on the model output, especially after seeing the change to the pseudo-random number generator constants (which means the prior RNG didn’t work). I ran the latest code in single threaded mode for the baseline scenario a couple of times, to establish that it was producing the same results (on my machine only), which it did. Then I ran the version from the initial import against the latest data, to control for data changes.
The resulting output tables were radically different to the extent that they appear incomparable, e.g. the older code outputs data for negative days and a different set of columns. Comparing by row count for day 128 (7th May) gave 57,145,154 infected-but-recovered people for the initial code but only 42,436,996 for the latest code, a difference of about 34%.
I wondered if the format of the data files had changed without the program being able to detect that, so then I reran the initial import code with the initial data. This yielded 49,445,121 recoveries – yet another completely different number.
It’s clear that the changes made over the past month and a half have radically altered the predictions of the model. It will probably never be possible to replicate the numbers in Report 9.
Political attention. I was glad to see the analysis was read by members of Parliament. In particular, via David Davis MP the work was seen by Steve Baker – one of the few British MPs who has been a working software engineer. Baker’s assessment was similar to that of most programmers: “David Davis is right. As a software engineer, I am appalled. Read this now”. Hopefully at some point the right questions will be asked in Parliament. They should focus on reforming how code is used in academia in general, as the issue is structural incentives rather than a single team. The next paragraph will demonstrate that.
Do the bugs matter? Some people don’t seem to understand why these bugs are important (e.g. this computational biology student, or this cosmology lecturer at Queen Mary). A few people have claimed I don’t understand models, as if Google has no experience with them.
Imagine you want to explore the effects of some policy, like compulsory mask wearing. You change the code and rerun the model with the same seed as before. The number of projected deaths goes up rather than down. Is that because:The simulation is telling you something important?You made a coding error?The operating system decided to check for updates at some critical moment, changing the thread scheduling, the consequent ordering of floating point additions and thus changing the results?
You have absolutely no idea what happened.
In a correctly written model this situation can’t occur. A change in the outputs means something real and can be investigated. It’s either intentional or a bug. Once you’re satisfied you can explain the changes, you can then run the simulation more times with new seeds to estimate some uncertainty intervals.
In an uncontrollable model like ICL’s you can’t get repeatable results and if the expected size of the change is less than the arbitrary variations, you can’t conclude anything from the model. And exactly because the variations are arbitrary, you don’t actually know how large they can get, which means there’s no way to conclude anything at all.
I ran the simulation three times with the code as of commit 030c350, with the default parameters, fixed seeds and configuration. A correct program would have yielded three identical outputs. For May 7th the max difference of the three runs was 46,266 deaths or around 1.5x the actual UK total so far. This level of variance may look “small” when compared to the enormous overall projections (which it seems are incorrect) but imagine trying to use these values for policymaking. The Nightingale hospitals added on the order of 10-15,000 places, so the uncontrolled differences due to bugs are larger than the NHS’s entire crash expansion programme. How can any government use this to test policy?
An average of wrong is wrong. There appears to be a seriously concerning issue with how British universities are teaching programming to scientists. Some of them seem to think hardware-triggered variations don’t matter if you average the outputs (they apparently call this an “ensemble model”).
Averaging samples to eliminate random noise works only if the noise is actually random. The mishmash of iteratively accumulated floating point uncertainty, uninitialised reads, broken shuffles, broken random number generators and other issues in this model may yield unexpected output changes but they are not truly random deviations, so they can’t just be averaged out. Taking the average of a lot of faulty measurements doesn’t give a correct measurement. And though it would be convenient for the computer industry if it were true, you can’t fix data corruption by averaging.
I’d recommend all scientists writing code in C/C++ read this training material from Intel. It explains how code that works with fractional numbers (floating point) can look deterministic yet end up giving non-reproducible results. It also explains how to fix it.
Processes not people. This is important: the problem here is not really the individuals working on the model. The people in the Imperial team would quickly do a lot better if placed in the context of a well run software company. The problem is the lack of institutional controls and processes. All programmers have written buggy code they aren’t proud of: the difference between ICL and the software industry is the latter has processes to detect and prevent mistakes.
For standards to improve academics must lose the mentality that the rules don’t apply to them. In a formal petition to ICL to retract papers based on the model you can see comments “explaining” that scientists don’t need to unit test their code, that criticising them will just cause them to avoid peer review in future, and other entirely unacceptable positions. Eventually a modeller from the private sector gives them a reality check. In particular academics shouldn’t have to be convinced to open their code to scrutiny; it should be a mandatory part of grant funding.
The deeper question here is whether Imperial College administrators have any institutional awareness of how out of control this department has become, and whether they care. If not, why not? Does the title “Professor at Imperial” mean anything at all, or is the respect it currently garners just groupthink?
Insurance. Someone who works in reinsurance posted an excellent comment in which they claim:There are private sector epidemiological models that are more accurate than ICL’s.Despite that they’re still too inaccurate, so they don’t use them.“We always use 2 different internal models plus for major decisions an external, independent view normally from a broker. It’s unbelievable that a decision of this magnitude was based off a single model“
They conclude by saying “I really wonder why these major multinational model vendors who bring in hundreds of millions in license fees from the insurance industry alone were not consulted during the course of this pandemic.“
A few people criticised the suggestion for epidemiology to be taken over by the insurance industry. They had insults (“mad”, “insane”, “adding 1 and 1 to get 11,000” etc) but no arguments, so they lose that debate by default. Whilst it wouldn’t work in the UK where health insurance hardly matters, in most of the world insurers play a key part in evaluating relative health risks.
![]() by alloneword » Mon May 11, 2020 9:57 am
by alloneword » Mon May 11, 2020 9:57 am
OUR PLAN TO REBUILD: The UK Government’s COVID-19 recovery strategy
![]() by alloneword » Mon May 11, 2020 10:20 am
by alloneword » Mon May 11, 2020 10:20 am
alloneword » Wed May 06, 2020 5:05 pm wrote:I'm looking at the UK's 'Scientific Advisory Group for Emergencies', (so modestly abbreviated to 'SAGE') - the group from which the freshly disgraced Mr. Ferguson has decided to 'step back'.
Many (but by no means all) of the documents comprising the 'Scientific evidence supporting the [UK] government response to COVID-19' are now available here:
https://www.gov.uk/government/groups/sc ... o-covid-19
An index (xls) file here: https://assets.publishing.service.gov.u ... papers.csv gives further indications as to what has - and perhaps more importantly, hasn't - been published.
Some of this stuff, they've taken over 3 months to publish, much of it they probably never will.
UK scientists condemn 'Stalinist' attempt to censor Covid-19 advice
Government scientific advisers are furious at what they see as an attempt to censor their advice on government proposals during the Covid-19 lockdown by heavily redacting an official report before it was released to the public, the Guardian can reveal.
[...]
One SPI-B adviser said: “It is bloody silly, and completely counterproductive.” A second committee member said: “The impression I’m getting is this government doesn’t want any criticism.”
On Friday afternoon, after the Guardian revealed frustrations over the redacted report, another member of the government’s advisory committee took to Twitter to complain of what he said was “Stalinist” censorship.
“Personally, I am more bemused than furious,” said Stephen Reicher, a professor of social psychology at the University of St Andrews. “The greatest asset we have in this crisis is the trust and adherence of the public. You want trust? You need to be open with people. This isn’t open. It is reminiscent of Stalinist Russia. Not a good look.”
Members of the committee have been discussing among themselves how best to respond to the redaction, which they believe was a heavy-handed move that jeopardises their independence.
At least one scientific adviser is understood to be considering resigning over the government’s secretive approach to science around the Covid-19 outbreak, which they believe is undermining public trust.
The report, from 1 April, summarised SPI-B’s discussions about how to handle possible changes to the social distancing measures that had just been introduced to slow the spread of Covid-19.
In the version published on Sage’s government website, almost a page and a half of text was heavily redacted. The Guardian understands the blocked text related to SPI–B’s criticism about possible government proposals around that time.
These included the idea of reducing the amount of time Britons could spend exercising or shopping, and stricter financial penalties for those found to be breaking the lockdown. A third proposal involved requiring people to self-validate their movements, as was occurring in France, where citizens were required to complete permits before leaving home...
![]() by alloneword » Mon May 11, 2020 10:45 am
by alloneword » Mon May 11, 2020 10:45 am

3. Specific comments about new suggestions for improving adherence within the
Framework (27 March)
The Framework proposes four new suggestions for increasing adherence, numbered as options 17 to
20 that SPI-B have not commented on before. These focus on: 17) increasing the financial penalties
imposed; 18) introducing self-validation for movements; 19) reducing exercise and/or shopping; 20)
reducing non-home working.
We have reservations about options 17 to 19. First, we are unclear what the evidence base is that
the targeted behaviours are a substantial contribution to disease transmission, particularly given the
high adherence rates currently observed in the community. Is there evidence, for example, that
exercise conducted more than 1km away from the house leads to higher rates of transmission than
exercise conducted within 1km of the house? Indeed, for this option, there is a risk that reducing the
ability of people to apply some flexibility in choosing where to exercise will increase risk by
preventing people from spreading out in nearby open space. Tightening restrictions without clear
epidemiological need may lose support among people who have been attempting to adhere.
Second, the implicit assumption underlying options 17 to 19 is that people lack motivation to adhere
to current guidance. This may apply to some specific subgroups (the example of young men has
been given), but broadly the current levels of adherence we are witnessing suggest this is not the
issue.
Third, there are equity issues within options 17 to 19. Any flat rate financial penalty will have a
higher impact on poorer households, while the assumption that printing and completing paperwork
is straightforward for all households can also be challenged. The assumption underlying restrictions
on shopping frequency is that people can afford to buy in larger quantities. The risk of tension arising
as the police are required to start penalising those who are not adhering should also be factored into
considerations.
With regards to option 20 (reduce home working), this appears to offer more room to reduce
contacts in the community, given that 13% of those polled by YouGov report still going to their place
of work as much as usual. However, the success of this strategy is contingent on financial support
reaching those who are furloughed in a timely manner, or else there is a risk of tension resulting for
a lack or equity in this measure.
We would also propose two additional suggestions that might be considered.
First, we note that the new suggestions proposed in the Framework are based on additional
restrictions, barriers or punishments. We recommend that HM Government also consider the role of
rewards and facilitations in improving adherence. Rapid research will be needed to inform this –
what are the reasons why people are finding it difficult to adhere to current advice? But as
examples, consideration could be given to providing quicker access to financial support so that
people do not feel compelled to attend work or free home entertainment or on-line education (in
partnership with industry bodies) to provide an alternative to leaving home when bored.
Second, we note that the additional suggestions largely operate at the level of the individual. We
recommend that consideration also be given to ways to reduce disease transmission at a more
organisational level. Are health and safety guidelines adequate (and adequately enforced) to ensure
that where people do attend work, the risk of disease transmission is minimised by, for example,
allowing sufficient breaks and facilities for hand hygiene, staggered office hours to reduce rush hour
use of public transport, or enough space and guidance to allow within-work physical distancing?
![]() by alloneword » Mon May 11, 2020 11:25 am
by alloneword » Mon May 11, 2020 11:25 am
Of bits, bugs and responsibility in the public square
By Chris von Csefalvay 2 days ago
Usually, I wake to the sound of the bluejays in our spacious backyard. This morning, I woke to the ‘priority alert’ from my phone, indicating an urgent message. It was 0515 – early even by the standards of epidemiologists in these times. My friend’s message was terse but foreboding – “look at this”, followed by a link to Github.
At the end of the link was the codebase promised for weeks by Neil Ferguson, the computational epidemiologist who has advised the UK government on COVID-19 related steps until his recent resignation. I have previously been a staunch defender of Ferguson’s approach – his model was (and is) theoretically sound, and probably as good as such models will ever get. Prediction, of course, is difficult. Especially when it comes to the future, as Niels Bohr is credited of saying. Using a method that relies on simulating populations in cells and microcells, it combines the granularity and stochastics of agent-based models without requiring the resources typical for agent-based simulation. His model, versions of which were used in previous outbreaks, has been the de facto gold standard to the UK government.
And looking at the code, that raises some extremely serious questions. I would like to explore some of these issues, but will not go into a detailed analysis of the code, for one reason – the code eventually (and reluctantly) shared by Imperial College is almost definitely not the code used to generate forecasts for HM Government. We know that at some point, Github and even John Carmack (yes, that John Carmack!) has been involved in cleaning up some of the quality issues. Imperial, meanwhile, obstinately resists releasing original code – both via Github and under a valid FOIA request that Imperial’s lawyers are entirely misinterpreting.1) We can, however, safely assume from the calibre of the people who have worked on the improved version that whatever was there was worse.
The quality issue
First of all, the elephant in the room: code quality. It is very difficult to look at the Ferguson code with any understanding of software engineering and conclude that this is good, or even tolerable. Neil Ferguson himself attempts a very thin apologia for this:
That, sir, is not a feature. It’s not even a bug. It’s somewhere between negligence and unintentional but grave scientific misconduct.
For those who are not in the computational fields: “my code is too complicated for you to get it” is not an acceptable excuse. It is the duty of everyone who releases code to document it – within the codebase or outside (or a combination of the two). Greater minds than Neil Ferguson (with all due respect) have a tough enough time navigating a large code base, and especially where you have collaborators, it is not unusual to need a second or two to remember what a particular function is doing or what the arguments should be like. Or, to put it more bluntly: for thirteen years, taxpayer funding from the MRC went to Ferguson and his team, and all it produced was code that violated one of the most fundamental precepts of good software development – intelligibility.
The policy issue
When you write code, you should always do so as if your life depended on it. For us working in the field of modelling infectious diseases, lives being at stake is common, sometimes to the point of losing track of it. I don’t, of course, know whether that is what indeed happened, but I doubt anybody would want to trust their lives to thousands of lines of cobbled-together code.
Yet for some reason, the UK government treated Ferguson’s model as almost dogmatic truth. This highlights an important issue: politicians have not been taught enough about data-driven decision-making, especially not where predictive data is involved. There is wide support for a science-driven response to COVID-19, but very little scrutiny of the science behind many of the predictions that informed early public health measures. Hopefully, a Royal Commission with subpoena powers will have the opportunity to review in detail whether Ferguson intentionally hid the model from HM Government the way he hid it from the rest of the world or whether the government’s experts just did not understand how to scrutinise or assess a model – or, the worst case scenario: they saw the model and still let it inform what might have been the greatest single decision HM Government has made since 1939, without looking for alternatives (there are many other modelling approaches, and many developers who have written better code).
The community issue
Perhaps the biggest issue is, however, the response to people who dare question the refusal by Imperial to release the original source code. This is best summarised by the responses of their point man on Github, who is largely spending his time locking issues and calling people dumb & toxic:
It may merit attention that the MRC is taxpayer-funded – the self-same taxpayer who is deemed unfit to even behold what he paid for. This is the worst of ‘closed science’, something many scientists (myself included) have worked hard to dismantle over the years. Publicly funded science imposes a moral obligation to present its results to the funder (that is, the taxpayer), and it should perhaps not be up to the judgment of a junior tech support developer to determine what the public is, or is not, fit to see. Perhaps as an epidemiologist, I take special umbrage at the presumption that everyone who wishes to see the original code base would be “confused” – maybe I should write to reassure Dr Hinsley that I do understand a little about epidemiology. It is, after all, what I do.
The science issue
None of these issues are, of course, anywhere near as severe as what this means – a massive leap backwards, erosion of trust and a complete disclaimer of accountability by publicly funded scientists.
There is a moral obligation for epidemiologists to work for the common good – and that implies an obligation of openness and honesty. I am reminded of the medical paternalism that characterised Eastern Bloc medicine, where patients were rarely told what ailed them and never received honest answers. To see this writ large amidst a pandemic by what by all accounts (mine included) has been deemed one of the world’s best computational epidemiology units is not so much infuriating as it is deeply saddening.
One of my friends, former Navy SEAL Jocko Willink, counseled in his recent book to “take the high ground, or the high ground will take you”. Epidemiology had the chance to seize and hold the narrative, through openness, transparency and honesty about the forecasts made. It had the chance, during this day in the sun of ours, to show the public just how powerful our analytical abilities have become. Instead, petty academic jealousy, obsessions with institutional prestige and an understandable but still disproportionate fear of being ‘misinterpreted’ by people who ‘do not understand epidemiology’ have given the critics of forecasting and computational epidemiology fertile breeding ground. They are entirely justified now in criticising any forecasts that come out of the Imperial model – even if the forecasts are correct. There will no doubt be public health consequences to the loss of credibility the entire profession has suffered, and in the end, it’s all due to the outdated ‘proprietary’ attitudes and the airs of superiority by a few insulated scientists who, somehow, somewhere, left the track of serving public health and humanity for the glittering prizes offered elsewhere. With their abandonment of the high road, our entire profession’s claim to the public trust might well be forfeited – in a sad twist of irony, at a time that could well have been the Finest Hour of computational epidemiology.
And while we may someday regain the respect of the public we swore to serve (perhaps after a detailed inquiry into what went wrong), for now there will be never glad confident morning again.
References
1. ↑ Section 22A allows for non-disclosure of ongoing research if it is in the public interest. It’s not that I disagree with Imperial on whether it’s in the public interest or not to release the code: it’s that I cannot for the life of me see how anyone could reasonably consider that it is not. Which just so happens to be the administrative law standard when adjudicating issues like this.
![]() by alloneword » Mon May 11, 2020 11:38 am
by alloneword » Mon May 11, 2020 11:38 am
![]() by JackRiddler » Tue May 12, 2020 4:37 pm
by JackRiddler » Tue May 12, 2020 4:37 pm
More than one in five people who were tested for virus antibodies in N.Y.C. had them.
More than 21 percent of around 1,300 people in New York City who were tested for coronavirus antibodies this week were found to have them, Gov. Andrew M. Cuomo said on Thursday.
The results were from a state program that tested 3,000 supermarket customers across New York State. Nearly 14 percent of the tests came back positive, Mr. Cuomo said.
It was unclear just how telling the preliminary data was, as Mr. Cuomo acknowledged. And the accuracy of the antibody testing available in the United States in general has been called into question.
Antibody tests are intended to signal whether a person may have built immunity to virus. They do not test for the virus itself.
But if the state’s numbers indicated the true incidence of the virus, they would mean that more than 1.7 million people in New York City, and more than 2.6 million people statewide, have already been infected.
That is far greater than the 250,000 confirmed cases of the virus itself that the state has recorded.
It would also mean that the fatality rate from the virus was relatively low, about 0.5 percent, Mr. Cuomo said.
Video
Back
0:00/1:35
TRANSCRIPT
Antibody Tests Show High Infection Rate for New York City
About 21 percent of people in New York City who were tested for coronavirus antibodies tested positive, Gov. Andrew M. Cuomo said.
So we have undertaken the largest, most comprehensive study of New York State to find out what is the infection rate. And that we started a few days ago. Sample size, so far, 3,000 people statewide. Let’s find out what the infection rate is. We have preliminary data on Phase 1, and this is going to be ongoing. We did about 3,000 tests. But what we found so far is the statewide number is 13.9 percent tested positive for having the antibodies. What does that mean? It means these are people who were infected, and who developed the antibodies to fight the infection. Long island at 16.7, New York City at 21.2 Westchester/Rockland, 11.7 and rest of state, 3.6. This basically quantifies what we’ve been seeing anecdotally, and what we have known, but it puts numbers to it. It changes the theories of what the death rate is. If you get infected, 13 percent of the population is about 2.7 million people who have been infected. If you look at what we have now as a death total, which is 15,500, that would be about 0.5 percent death rate.
1:34
Antibody Tests Show High Infection Rate for New York City
About 21 percent of people in New York City who were tested for coronavirus antibodies tested positive, Gov. Andrew M. Cuomo said.CreditCredit...Cindy Schultz for The New York Times
Hours before Mr. Cuomo’s presentation, a top New York City health official cautioned against relying heavily on antibody tests in making critical decisions about social distancing and reopening the economy, particularly in identifying immunity.
The city’s top disease control official, Dr. Demetre C. Daskalakis, wrote in an email alert on Wednesday that the tests “may produce false negative or false positive results,” pointing to “significant voids” in using the science to pinpoint immunity.
Mr. Cuomo declined to speculate on what the preliminary data might mean. He said its main use would be to provide a baseline for tracking changes in the infection rate.
Supermarket customers do not constitute a random sample of the population. On one hand, they are out in public and spending time in stores, which could increase their exposure to the virus.
On the other hand, they are presumably not actively sick, or living in nursing homes, where the virus has taken a heavy toll. And, of course, no one who was killed by the virus was tested for antibodies.
“What does it mean? I don’t know,” Mr. Cuomo said. “These are people who were out and about shopping. They were not people who were in their homes, they were not people who were isolated, they were not people who were quarantined.”
TANTALIZING DATA Preliminary data from antibody tests indicated that many New Yorkers who did not know it may have survived the virus already.
https://www.nytimes.com/2020/04/23/nyre ... ve-updates
A Coronavirus Death in Early February Was ‘Probably the Tip of an Iceberg’
The startling discovery that the virus was responsible for a Feb. 6 death in California raises questions about where else it might have been spreading undetected.
The coronavirus was circulating in the Bay Area of California as early as January, even before the federal government began restricting travel from China on Feb. 2.
The coronavirus was circulating in the Bay Area of California as early as January, even before the federal government began restricting travel from China on Feb.
By Thomas Fuller, Mike Baker, Shawn Hubler and Sheri Fink
April 22, 2020
阅读简体中文版閱讀繁體中文版
SAN FRANCISCO — Weeks before there was evidence that the coronavirus was spreading in U.S. communities, Patricia Dowd, a 57-year-old auditor at a Silicon Valley semiconductor manufacturer, developed flulike symptoms and abruptly died in her San Jose kitchen, triggering a search for what had killed her. Flu tests were negative. The coroner was baffled. It appeared that she had suffered a massive heart attack.
But tissue samples from Ms. Dowd, who died on Feb. 6, have now shown that she was infected with the coronavirus — a startling discovery that has rewritten the timeline of the virus’s early spread in the United States and suggests that the optimistic assumptions that drove federal policies over the early weeks of the outbreak were misplaced [...]
71,000 Missing Deaths:
Tracking the True Toll of the Coronavirus Outbreak
By Jin Wu, Allison McCann, Josh Katz and Elian PeltierUpdated May 12, 2020, 3:30 P.M. E.T.
https://www.nytimes.com/interactive/202 ... Position=2
What 5 Coronavirus Models Say the Next Month Will Look Like
By Quoctrung Bui, Josh Katz, Alicia Parlapiano and Margot Sanger-KatzApril 22, 2020
https://www.nytimes.com/interactive/202 ... odels.html
A Marm Kilpatrick
@DiseaseEcology
Stanford Serology study preprint just posted that is certain to mislead many people:
https://medrxiv.org/content/10.1101/202 ... 1.full.pdf
It's a serological study, which is fantastic. We need these kinds of studies and data badly. Unfortunately this paper is badly misleading (bordering on purposeful?)
3:05 PM · Apr 17, 2020·Twitter Web App
319
Retweets
663
Likes
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
Replying to
@DiseaseEcology
It recruits people via Facebook ads which are clearly not a random sample of the population. The most important subject trait given the influence of age on COVID-19 mortality is: AGE! And yet this study does not present seroprevalence by age or adjust its estimates by age.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
It doesn't even present information on the study cohort in enough detail to see the differences in frequency b/w ages of the sample and the pop. They group all19-64 year olds! And there is no measurement of socio-economic status. Both factors (age, $$) likely affect exposure.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
There are also questions with the test performance. The manufacturer reported 100% sensitivity for known IgG positives from elisa (75/75) and 92% (78/85) for IgM known +. When they ran the test on samples from Stanford, sensitivity was 68% (25/37) not broken down by IgG/IgM.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
Specificity was better (369/371 from manufacturer, 30/30 at Stanford). Poorer sensitivity elevates estimates of True seroprevalence, which leads to their highest estimate: 4.16%.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
What should we (safely) conclude from this preprint? I think it's very challenging to interpret the data at all without showing seroprev by age. If seroprev is higher for young people then exposure of old people could be lower.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
This matters b/c mortality is ~0 for 0-40 age. Older individs >65 were 3-fold underestimated in survey, so applying their corrected estimates this group would be very problematic.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
I've posted comments on the preprint page asking authors to breakdown data by age and adjust for age. If they do, we can get much more from this study. But they didn't even try to collect data on socioeconomic factors and they didn't adjust their results based on prior symptoms.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
Perhaps most important, it seems likely that individuals that had COVID-19 symptoms would be more likely to volunteer to be tested and this could lead to substantial overestimate of seroprevalence. Prev symptoms data were collected but not discussed (???).
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
Conclusion: do NOT interpret this study as an accurate estimate of the fraction of population exposed. Authors have made no efforts to deal with clearly known biases and whole study design (recruiting via FB ad? Really?) is problematic.
A Marm Kilpatrick
@DiseaseEcology
·
Apr 17
Addendum - it would also have been nice to know the professions of sampled individs vs gen. pop. Some jobs likely have much higher exposure. This could also greatly influence results.
The Pandemic’s Hidden Victims: Sick or Dying, but Not From the Virus
As the coronavirus overwhelms the health care system, people with other illnesses struggle to find treatment.
Dr. Bruce Lowell, an internist in Great Neck, N.Y. “People are still having heart attacks, people are still having strokes,” he said. “I feel as if there is no awareness of anything other than Covid.”
By Denise Grady
April 20, 2020
https://www.nytimes.com/2020/04/20/heal ... virus.html
Coronavirus antibody testing shows LA County outbreak is up to 55 times bigger than reported cases
PUBLISHED MON, APR 20 2020
UPDATED TUE, APR 21 2020
Noah Higgins-Dunn
@HIGGINSDUNN
Hannah Miller
The Covid-19 outbreak in Los Angeles County could be up to 55 times bigger than the number of confirmed cases, according to new research from the University of Southern California and the LA Department of Public Health.
The data, if correct, would mean that the county’s fatality rate is lower than originally thought.
With just 4% of the population infected with the disease, LA County is still very early in the epidemic, said USC professor Neeraj Sood, who led the study
The Covid-19 outbreak in Los Angeles County is likely far more widespread than previously thought, up to an estimated 55 times bigger than the number of confirmed cases, according to new research from the University of Southern California and the LA Department of Public Health.
USC and the health department released preliminary study results that found that an estimated 4.1% of the county’s adult population has antibodies to the coronavirus, estimating that between 221,000 adults to 442,000 adults in the county have had the infection.
This new estimate is 28 to 55 times higher than the 7,994 confirmed cases of Covid-19 reported to the county through early April. The number of coronavirus-related deaths in the county has now surpassed 600, according to the Department of Public Health. The data, if correct, would mean that the county’s fatality rate is lower than originally thought.
The results are based on antibody testing of about 863 people who were representative of LA County, the researchers said.
“Though the results indicate a lower risk of death among those with infection than was previously thought, the number of Covid-related deaths each day continues to mount, highlighting the need for continued vigorous prevention and control efforts,” said Dr. Paul Simon, chief science officer at the LA County Department of Public Health and co-lead on the study, in a statement.
[...]
Nearly a third of 200 blood samples taken in Chelsea show exposure to coronavirus
Mass. General researcher says the results point to a ‘raging epidemic,’ but may also indicate the city is further along the disease curve than some other municipalities
By Jonathan Saltzman
Globe Staff,Updated April 17, 2020, 6:26 p.m.
Nearly one third of 200 Chelsea residents who gave a drop of blood to researchers on the street this week tested positive for antibodies linked to COVID-19, a startling indication of how widespread infections have been in the densely populated city.
Sixty-four residents who had a finger pricked in Bellingham Square on Tuesday and Wednesday had antibodies that the immune system makes to fight off the coronavirus, according to Massachusetts General Hospital physicians who ran the pilot study.
The 200 participants generally appeared healthy, but about half told the doctors they had had at least one symptom of COVID-19 in the past four weeks.
Public health experts already knew Chelsea had the state’s highest rate of confirmed COVID-19 cases and that the actual rate was probably higher. At least 39 residents have died from the virus, and 712 had tested positive as of Tuesday, a rate of about 1,900 cases per 100,000 residents, or almost 2 percent.
But the Mass. General researchers ― who excluded anyone who had tested positive for the virus in the standard nasal swab test ― found that 32 percent of participants have had COVID-19, and many didn’t know it.
“I think it’s both good news and bad news,” said Dr. John Iafrate, vice chairman of MGH’s pathology department and the study’s principal investigator. “The bad news is that there’s a raging epidemic in Chelsea, and many people walking on the street don’t know that they’re carrying the virus and that they may be exposing uninfected individuals in their families.”
RELATED: Opinion | Chelsea, city of the working Latino immigrant, emerges as a COVID-19 hotspot
“On the good-news side, it suggests that Chelsea has made its way through a good part of the epidemic,” he said. “They’re probably further along than other towns.”
Scientists suspect that people who recover from COVID-19 may be at least temporarily immune from catching it again. Several biotechs and academic laboratories, in fact, are seeking blood donations from people who have recovered, in the hopes that their antibodies can help create a treatment or vaccine.
Chelsea’s city manager, Thomas Ambrosino, said he learned the results of the pilot study Thursday in a conference call with the researchers. He was dismayed, but not shocked.
RELATED: Chelsea city manager sounds urgent alarm, calls for residents to stay home 24 hours a day
“We’ve long thought that the reported numbers are vastly under-counting what the actual infection is,” said Ambrosino, who has called his city the epicenter of the crisis in Massachusetts. “Those reported numbers are based on positive COVID-19 tests, and we’re all aware that a very, very small percentage of people in Chelsea and everywhere are getting COVID-19 tests.”
“Still,” he added, “it’s kind of sobering that 30 percent of a random group of 200 people that are showing no symptoms are, in fact, infected. It’s all the more reason for everyone to be practicing physical distancing.”
Indeed, one of the doctors who tested volunteers in Bellingham Square said it’s possible that some of the people who had the antibodies are still contagious.
“Just because you have the antibodies doesn’t mean you’ve cleared the virus,” said Dr. Vivek Naranbhai, a clinical fellow in hematology and oncology.
Researchers said the test results, which had yet to be shared with state officials late Friday, couldn’t necessarily be extrapolated for the city’s roughly 40,000 residents. Still, the findings provided a valuable snapshot of a community that medical experts say is especially vulnerable to COVID-19.
Chelsea covers only about two square miles, across the Mystic River from Boston. For generations, it has attracted new immigrants, and about 65 percent of its residents are Latino. Many live in three-decker houses, Ambrosino said, where it’s hard for people to isolate themselves. Many work in the hospitality industry and health-related fields, where exposure to the virus is greater. And a lot of them must go to work during the pandemic.
To get Chelsea residents to participate in the study ― which included a questionnaire that was available in English, Spanish, and Portuguese — investigators allowed them to remain anonymous. But that meant none of the participants received the results of the blood tests.
The doctors used a diagnostic device made by BioMedomics, of Morrisville, N.C., to analyze drops of blood. It resembled an over-the-counter pregnancy test and generated results on the street in about 10 minutes. Although the test hasn’t won the approval of the Food and Drug Administration, Iafrate, the principal investigator, said Mass. General determined it’s reliable.
Within days, the physicians said, they hope to set up a medical tent outside the Mass. General Chelsea Healthcare Center to perform more antibodies tests with the device. The site will be located near a tent set up weeks ago to run standard PCR, or polymerase chain reaction, tests for people with active coronavirus symptoms. The latter uses nasal swabs to detect whether the virus is present at the time; the antibodies blood test reveals whether someone was infected in the past.
In addition to the new testing site, the researchers want to expand the study to other Massachusetts cities and towns. For all of those studies, Mass. General doctors plan to obtain the identities of participants so physicians can provide the results. But first the researchers need to come up with guidelines for what participants should do if they test positive for antibodies.
Dr. Dean Xerras, medical director of the Mass. General Chelsea Healthcare Center and a co-investigator in the study, said it illustrates why it’s essential for Chelsea and other communities to perform more tests, regardless of whether they detect antibodies or the virus itself.
“Knowing how many people are infected is critical,” said Xerras, a longtime member of the city’s board of health. “We need to get them isolated. We need to get masks delivered to the city. We need to launch more safe isolation sites. We need to be able to identify cases and then give people the things they need to prevent perpetuation of the spread.”
Chelsea and Revere officials, with help from the state Department of Public Health and the Massachusetts Emergency Management Agency, secured almost 150 rooms at a Quality Inn in Revere this week for residents who are recovering from COVID-19 and unable to isolate themselves at home, according to Ambrosino. So far, only a handful of those rooms are occupied.
Governor Charlie Baker on Thursday staunchly defended the state’s handling of the escalating outbreak in Chelsea, including asserting, without offering details, that city leaders have turned down help from his administration.
With Broad, Random Tests for Antibodies, Germany Seeks Path Out of Lockdown
It was the first large Western democracy [why is this in the headline?] to contain the spread of the coronavirus and is now the first to methodically go about reopening its economy. Others are watching.
Taking a blood sample as part of random sampling for antibodies to the coronavirus.Credit...
By Katrin Bennhold
Published April 18, 2020
Updated April 20, 2020
https://www.nytimes.com/2020/04/18/health/cdc-coronavirus-lab-contamination-testing.html
C.D.C. Labs Were Contaminated, Delaying Coronavirus Testing, Officials Say
Fallout from the agency’s failed rollout of national coronavirus kits two months ago continues to haunt U.S. efforts to combat the spread of the highly infectious virus.
https://www.nytimes.com/2020/04/19/us/c ... tests.html
Antibody Test, Seen as Key to Reopening Country, Does Not Yet Deliver
The tests, many made in China without F.D.A. approval, are often inaccurate. Some doctors are misusing them. The rollout is nowhere close to the demand.
![]() by alloneword » Thu May 14, 2020 2:11 pm
by alloneword » Thu May 14, 2020 2:11 pm
Covid-19: What is the evidence for cloth masks?
BMJ 2020; 369 doi: https://doi.org/10.1136/bmj.m1422 (Published 07 April 2020) Cite this as: BMJ 2020;369:m1422
Elisabeth Mahase
As the US Centers for Disease Control and Prevention has advised all Americans to wear cloth masks in public to prevent the spread of covid-19, The BMJ examines the evidence
What has the CDC recommended?
People should wear cloth face coverings in public places where social distancing measures are “difficult to maintain,” such as supermarkets and pharmacies, the CDC advises. It said the masks can be “fashioned from household items or made at home from common materials at low cost.” It also warned that surgical masks and N-95 respirators should not be used by the public, as these were “critical supplies that must continue to be reserved for healthcare workers and other medical first responders.”
How do you make a homemade cloth mask?
The CDC recommends using tightly woven cotton fabric, such as quilting fabric, cotton sheets, or T shirt fabric. It provided instructions on how to make masks with or without sewing, including using a bandana and coffee filter to create a face covering.1
But are they effective?
Very little good quality research exists on the use of cloth masks, especially in non-medical settings. One randomised controlled clinical trial of cloth masks, published in BMJ Open in 2015, compared their effectiveness with that of medical masks worn by hospital healthcare workers.2 The study, involving the industry partner 3M (which makes medical masks), reported that healthcare workers “should not use cloth masks as protection against respiratory infection. Cloth masks resulted in significantly higher rates of infection than medical masks, and also performed worse than the control arm.”
In an updated comment on the study (30 March),3 the authors said, “There have been a number of laboratory studies looking at the effectiveness of different types of cloth materials, single versus multiple layers and about the role that filters can play. However, none have been tested in a clinical trial for efficacy.”
They also advised healthcare workers who choose to wear cloth masks to “have at least two and cycle them, so that each one can be washed and dried after daily use. Sanitizer spray or UV disinfection boxes can be used to clean them during breaks in a single day. These are pragmatic, rather than evidence-based suggestions, given the situation.”
A preprint of a rapid systematic review has assessed the current evidence on respiratory illnesses and the use of face masks (mainly surgical paper masks) in community settings.4 The paper, yet to be peer reviewed, included 31 studies, of which 12 were randomised controlled trials. The researchers reported that “wearing facemasks can be very slightly protective against primary infection from casual community contact, and modestly protective against household infections when both infected and uninfected members wear facemasks.” However, they said that many of the studies “suffered from poor compliance and controls.”
They concluded, “The evidence is not sufficiently strong to support widespread use of facemasks as a protective measure against covid-19. However, there is enough evidence to support the use of facemasks for short periods of time by particularly vulnerable individuals when in transient higher risk situations.”
Commenting on these findings, Simon Clarke, associate professor in cellular microbiology at the University of Reading, said, “There is only very limited evidence of the benefits of wearing face masks by the general public, no evidence that wearing them in crowded places helps at all, and no evidence at all yet related to covid-19 . . . The authors also acknowledge that mass face mask wearing by the public would likely cause shortages among people who genuinely need protective equipment—healthcare workers on the front line in our hospitals.”
But Ian Jones, professor of virology at the University of Reading, said, “If an aerosol droplet hits the weave of the mask fabric rather than the hole it is clearly arrested. And lessening the aerosol dose chips away at the R0 [reproduction number] and helps to slow the epidemic . . . They are not a cure but they address the longer flatter epidemic curve everyone is trying to achieve.”
Have other countries recommended masks for the public?
Israel, Austria, the Czech Republic, Hong Kong, and Mongolia are among the countries that have implemented or recommended mask wearing in the community.
Could it have negative effects?
Experts have warned that recommending that members of the public wear masks can lead to shortages for those who are more in need: health and care workers and immunocompromised people, for example. It can also lead to complacency.
Susan Michie, director of University College London’s Centre for Behaviour Change and a fellow of the Academy of Medical Sciences, said, “There are several explanations as to why face masks have not generally been found to be effective if worn by the general population: they do not protect against the virus getting into the eyes (only close fitting goggles do this); people may not fit the masks properly or take them on and off; and people may have a false sense of reassurance and thus pay less attention to other behaviours key to reducing transmission, such as social distancing and handwashing.”
This was echoed by the infectious disease physician Ben Killingley. He said there were several reasons why masks were not seen as being as effective in the community. These included that people “find it difficult to be compliant with mask use all of the time and that people may start wearing the masks too late.” The other problem, he said, was that the public did not have the resources to ensure safe mask use: changing them often, frequent hand hygiene, and removing and disposing of them safely.
Killingley added, “Face masks are not an infinite resource and should be reserved for when they are most effective. It would not be good if we were not able to provide masks to healthcare workers because the public had consumed supplies.”
What does WHO say?
In guidance issued on 6 April,5 WHO said that medical masks should be reserved for health workers. Most spread of the covid-19 virus is from known cases and requires contact with droplets from a cough or sneeze or infected surfaces. It said that “there is currently no evidence that wearing a mask (whether medical or other types) by healthy persons in the wider community setting, including universal community masking, can prevent them from infection with respiratory viruses, including covid-19.” Wearing masks in the community can also give people a false sense of security, it said, and lead to them neglecting other measures, such as hand hygiene and physical distancing.
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usage
References
1 ↵Centers for Disease Control and Prevention. Use of cloth face coverings to help slow the spread of COVID-19. https://www.cdc.gov/coronavirus/2019-nc ... rings.html
2 ↵MacIntyre CR, Seale H, Dung TC, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open2015;5:e006577. doi:10.1136/bmjopen-2014-006577. pmid:25903751 https://bmjopen.bmj.com/content/5/4/e00 ... f_ipsecsha
3 ↵ MacIntyre CR. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers[response]. BMJ Open2020;30. https://bmjopen.bmj.com/content/5/4/e00 ... ast-resort .pmid:25903751
PubMedGoogle Scholar
4 ↵Brainard JS, Jones N, et al. Facemasks and similar barriers to prevent respiratory illness such as COVID-19: a rapid systematic review. medRxiv 2020.04.01.20049528; doi:10.1101/2020.04.01.20049528.
https://www.medrxiv.org/content/10.1101 ... f_ipsecsha
5 ↵World Health Organization. Advice on the use of masks in the context of COVID-19. 6 Apr 2020. https://www.who.int/publications-detail ... (2019-ncov)-outbreak .
Return to Data & Research Compilations
Users browsing this forum: No registered users and 3 guests
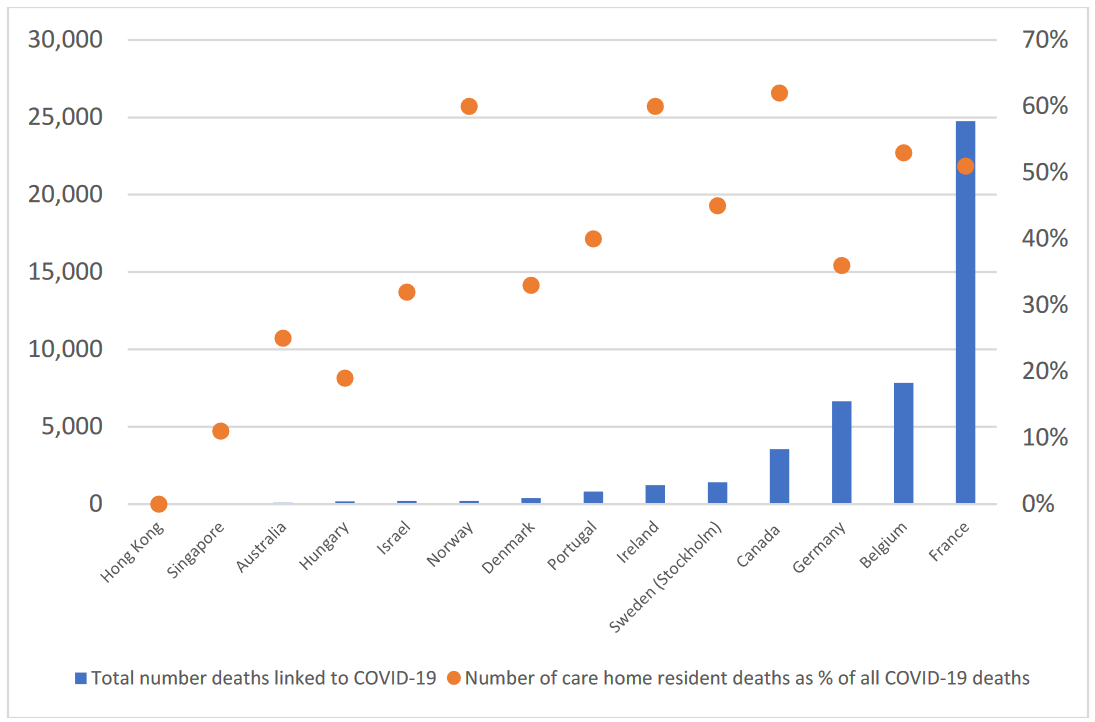





{kind=link}